Download
1 / 64
650 likes | 788 Vues
Infections of the Large Intestine. Pseudomembranous colitis and bacterial dysentery. To inflame or not to inflame. Antibiotic-associated pseudomembranous colitis 30% of hospitalized patients Clostridium difficile infects 5% of colons Resistant to many antibiotics

E N D
Infections of the Large Intestine Pseudomembranous colitis and bacterial dysentery
To inflame or not to inflame • Antibiotic-associated pseudomembranous colitis • 30% of hospitalized patients • Clostridium difficile infects 5% of colons • Resistant to many antibiotics • Antibiotics kill the good guys • Leaves C. difficile to overgrow
C. difficile • Etiology: • Anaerobe • Produces toxin A and toxin B
C. difficile • Symptoms • From asymptomatic to fulminant colitis • Depends on number of receptors for toxins on colon. • Watery diarrhea- most common (5-15 stools per day), crampy bilateral lower quadrant pain that decreases after bowel movement, low-grade fever, blood: leukocytosis • 5-10 days after antibiotic; can delay up to 10 wks
C. difficile • Symptoms • Pseudomembranous colitis- seen with colonoscopy; look for yellowish plagues
C. difficile • Symptoms • Fulminant colitis (2-3% of patients) • Usually diarrhea but can be constipated • Diffuse severe abdominal pain, hypoactive bowel sounds, abdominal distension and guarding • Marked peripheral blood leukocytosis • Complications: perforation, toxic megacolon
C. difficile • Pathology- not to inflame • Eliminate bacteria C. difficile overgrows • Watery diarrhea results due to undigested carbohydrate increase in ion in lumen
C. difficile • Pathology- to inflame • Toxins stimulate MAP-kinases and inactivate small GTP-binding Rho proteins • Toxins A and B cause cells to round up and die; shallow ulcers form • Inflammation follows • Pus and mucus accumulate resulting in pseudomembrane formation • Inflammation can extend through the entire bowel
C. difficile • Diagnosis • Hx antibiotic therapy • Used to think of clindamycin and lincomycin but any antibiotic can cause this disease. • ELISA for toxin A and B • 50% time stools have fecal leukocytes and are heme positive • Endoscopy; look for yellow plagues
C. difficile • Treatment • Withdraw antibiotic • Give intravenous fluid and electrolytes if severely dehydrated • NO ANTIMOTILITY DRUGS- increase chances for toxic megacolon and full-blown colitis • Metronidazole if needed • Megacolon: bowel resection and ileostomy
C. difficile • Prevention • Prevent spread to other patients and personnel. • Avoid prolonged use of broad-spectrum antibiotics.
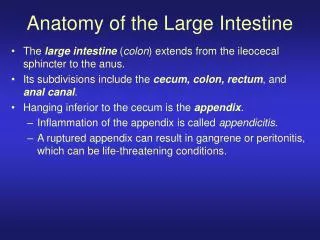
Bacterial Dysentery Invasive gastroenteritis Colitis, dysentery: to colonize and invade
Invasive Gastroenteritis • Affects large intestine; colon • Organisms invade • Cause host to mount inflammatory response • Stool volume small, contains mucus, leukocytes. • If deep enough blood can be in stool
Invasive Gastroenteritis • Usually fever • Abdominal pain • Pain while attempting to defecate (tenesmus) • Antibiotics can help • Exception; EHEC infections • Three most common causes: Campylobacter, Shigella, Salmonella
Invasive Gastroenteritis • Most common cause: Campylobacter • Other important causes • EHEC, EIEC, Yersinia enterocolitica, Entamoeba histolytica
Campylobacteriosis • Leading cause of bacterial diarrheal disease • 2 million cases per year • Isolated from cattle, chickens, birds and flies • Can be found in non-chlorinated water
Campylobacteriosis • Etiology • Campylobacter jejuni most common of eight species to cause colitis • S-shaped or comma shaped (seagull shape) • Hard to grow
Campylobacteriosis • Symptoms • Most cases are mild (7 d duration) • Initial symptoms • Periumbilical cramping • Intense abdominal pain • Malaise, myalgias, headache, vomiting • Watery diarrhea most common
Campylobacteriosis • Symptoms • Inflammatory bowel disease • Malaise, fever, abdominal cramps, tenesmus, bloody stool, fecal leukocytes • Indistinguishable from Shigella, Salmonella, E. coli.
Campylobacteriosis • Pathology • Adheres to epithelial and M cells • Heat-labile toxin- watery diarrhea • Invade cells- inflammatory colitis • Similar to Shigella and EIEC infections
Campylobacteriosis • Pathology • Invade cells- inflammatory colitis • Adhere to host cells • Use Type III secretory system to inject bacterial proteins • Host cell ruffles ingests bacteria • Shiga-toxin- stops protein synthesis • Kills cells • Superficial ulcers, inflammatory response
Campylobacteriosis • Diagnosis • See gull-shaped bacteria with darting motility in watery, bloody leukocyte-filled stool • Definitive: isolate bacteria from stool • Special media and isolation techniques • Campy-BAP or Skirrow media
Campylobacteriosis • Treatment • Most are self-limiting; no Rx • Oral rehydration; correct electrolyte imbalances • Do use antibiotic if patient has: • Fever • Increasing bloody diarrhea • Symptoms longer than a wk
Shigellosis • Fecal oral route of infection • Small numbers lead to infection • Around 300,000 cases per year • Only about 20,000-30,000 are reported per year • Problem in daycare, nursing homes, prisons • Can be spread to other via • Food • Fingers • Feces • Flies
Shigellosis • Etiology • Fifty species in 4 serologic groups • Only two serologic groups common in U.S. • Group D- S. sonnei most common in U.S. • Group B- S. flexneri • Nonmotile nonlactose fermenting gram-negative rod • Quite resistant to stomach acid
Shigellosis • Symptoms • Incubation 36-72 hrs • Fever, abdominal cramping and pain • Watery diarrhea • After 2 days of diarrhea then dysentery and tenesmus • May initiate septicemia by E. coli • Rarely gets into bloodstream
Shigellosis • Pathology • Adheres to M cells and epithelial cells • Use Type III secretory system to inject bacterial proteins • Host cell ruffling and ingest bacteria • Shigella uses hemolysin to lyse phagosome • In cytoplasm uses host actin to move inside cell.
Shigellosis • Pathology • When bacteria reach cell periphery it pushes outward • Membrane projections are formed • Ingested by adjacent cells • Meanwhile, Shiga toxin is killing cells by stopping protein synthesis • Cell to cell travel and destruction leaves superficial ulcers
Shigellosis • Pathology • An extensive inflammatory response occurs • The inflammatory response prevents systemic spread of the bacteria usually
Shigellosis • Diagnosis • Clinical symptoms- presumptive Dx • Definitive Dx- isolate organism from stools • Grow on S-S agar • Fecal leukocytes will be present
Shigellosis • Treatment • Usually self-limiting • To shorten course and limit person to person spread treat with antibiotics • Don’t give antidiarrheal compounds • Replace fluids and electrolytes • Prevention • Wash your hands
Salmonellosis • 2 to 4 million cases per year • Motile, nonlactose fermenting rod • Naming this genus has been a long debate • Over 2406 unique serogroups of Salmonella • Inhabit animals • From food, animals • Enteric fevers- person to person from chronic carriers
Salmonellosis • Etiology • I will use the genus name enterica for the non-enteric fever bacteria • S. enterica serotype typhimurium • Enteric fever- S. Paratyphi, S. Typhi • Typhoid fever and paratyphoid fever • http://www.pbs.org/wgbh/nova/typhoid/
Salmonellosis • Symptoms • Enteritis- most common- • Ingest food • 6-48 hr later nausea, abdominal cramps, vomiting, nonbloody diarrhea • Fever, headache, myalgia • Duration 2 d to 1 week • Usually self-limiting
Salmonellosis • Symptoms • Septicemia • All serovars can cause bacteremia • S. typhi, S. paratyphi A, S. enterica serovar choleraesuisS. schottmuelleri, S. hirschfeldii more likely • Higher risk in pediatric, geriatric, and immunocompromised populations • Just like any other gram-negative sepsis
Salmonellosis • Symptoms • Enteric fever • Typhoid fever- S. typhi • Paratyphoid fever- S. paratyphi A, S. schottmuelleri and S. hirschfeldii • Pass through lining of intestine • Engulfed by macrophages • Taken to liver, spleen, and bone marrow • Replicate
Salmonellosis • Symptoms • Enteric fever • 10-14 day later develop gradually rising fever • Fever lasts for a week or two • Then you see diarrhea • Can have skin lesions “rose spots” • Typhoid fever more severe than paratyphoid fever • Colonization of gallbladder can lead to a carrier state
Salmonellosis • Symptoms • Asymptomatic- enteric fever • Chronic colonization of the gallbladder • 1-5% of those infected • Can last up to a year
Salmonellosis • Pathology • Sensitive to stomach acid • Need large numbers for infection • Will attach to the epithelial cells cause ruffling • Bacteria are ingested and live in the vacuoles • Eventually lyse the cells
Salmonellosis • Pathology • After lysing the cells they get into the mesenteric lymph nodes • Can then get into the bloodstream • Can get nontyphoidal bacteremias • Get fever, abdominal pain, diarrhea • S. typhi and S. paratyphi cause very little damage in the intestine but rather are carried by WBCs to the bloodstream
Salmonellosis • Diagnosis • Less inflammation compared to shigellosis • Fewer leukocytes in the stool • Use S-S agar to isolate organisms
Salmonellosis • Treatment • Fluid replacement; NO antidiarrheals • Enteritis- is self-limiting. Treatment appears to prolong carriage and doesn’t shorten course of the illness • However, patients more likely to develop bacteremias should be treated • Enteric fever- antibiotic therapy immediately
Salmonellosis • Prevention • Travelers vaccination- for typhoid fever • Oral live attenuated • Vi capsular polysaccharide vaccine- IM
E. coli • EHEC and EIEC have obtained invasion genes from Shigella • Have many of the same capabilities and cause similar symptoms to Shigella
E. coli • EHEC- causes HC and can damage the kidneys resulting in HUS • Most common cause of HC and HUS is E. coli O157:H7 • Remember other non-O157:H7 serotypes can also cause HC and HUS
E. coli • Etiology • EIEC- invasion capabilities • EHEC- invasion capabilities and Shiga toxin • E. coli O157:H7- cannot ferment sorbitol