Download

1 / 1
10 likes | 253 Vues
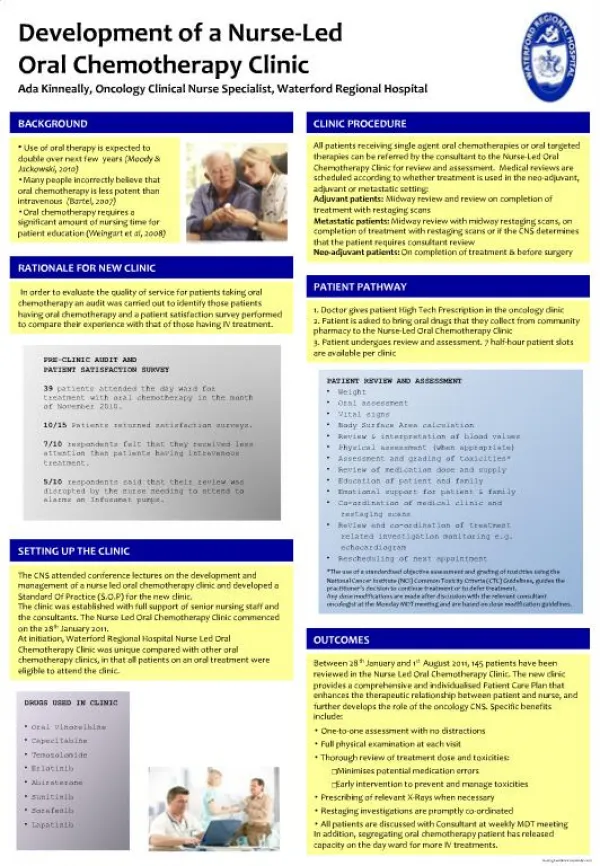
Hyponatraemia in Oncology: Magnitude of the problem: Proposed Management Algorithm for Syndrome of Anti Diuretic Hormone associated with Cancer A Joint Acute Oncology & Acute Medicine Project Bulusu V R, Jeffs Y P, Barclay C, Melvin A. Bedford Hospital Kempston Road, Bedford UK.

E N D
Hyponatraemia in Oncology: Magnitude of the problem: Proposed Management Algorithm for Syndrome of Anti Diuretic Hormone associated with Cancer A Joint Acute Oncology & Acute Medicine ProjectBulusu V R, Jeffs Y P, Barclay C, Melvin A. Bedford Hospital Kempston Road, Bedford UK Background: Hyponatraemia is defined as a serum Na+ of <135 mEq/l. SIADH secretion is a known metabolic complication of cancer resulting in hyponatraemia. Project designed to define the incidence of hyponatraemia and construct a management algorithm for SIADH. Traditional management of SIADH includes fluid restriction to < 1l/day, demeclocycline and hypertonic saline. Recently vasopressin-2 receptor antagonists have been introduced to treat SIADH. Methods: Serum sodium results from April to September 2011 extracted from the biochemistry database (N=31,420). Severe Hyponatraemia defined as serum sodium <125 mEq/l; results were coded against the requester’s speciality. Results: Severe hyponatraemia was documented in 447/31420, (1.4%) of all Na+ results. Biochemistry requests from Lung team (2.3%) and acute medicine team (3.3%) had the highest incidence. Full work up for SIADH was performed in <2%. We propose the following algorithm for cancer patients with SIADH. Management algorithm for SIADH in Oncology Hyponatraemia <135 mEq/l Serum Na+ <110mEq/l or acute neurological symptoms ITU Serum Na+ ≥125 mEq/l OBSERVE Hyponatraemia<125 mEq/l Serum Osmolality <270 mOsm Urine Osmolality >100 mOsmol Elevated Urinary Na+ >25 mEq/l Exclude ↓ T4 ↓ Cortisol Renal failure Euvolemic Acute Oncology & Endocrinology Jointly review management plan Acute Oncology Clinical Nurse Specialist Patient informed of Management plan SIADH • Information sheet for SIADH & consent • Review concomitant medications (drug interactions) • Oral Tolvaptan 15 mg od starting dose, ↑ to 60 mg as req • U/E LFTs on days 1, 3 and 5 • Continue Tolvaptan for 5-7 days & review • Specific anticancer treatment Conclusions: We propose a new management algorithm for the management of SIADH incorporating oral Tolvaptan, a vasopressin-2 receptor antagonist, avoiding the need for fluid restriction & demeclocyline. Patients with SIADH should be jointly managed by acute oncology and endocrinology specialist teams. vrbulusu@gmail.com