Exit
Cardiac Physiology. Chambers of the Heart. Anatomy of the heart. Pathology. Heart Physiology. Blood Flow Through the Heart. Mechanical Events during Heart Contraction. Electrocardiography. Heart Valves. Cardiac Muscle. Blood Flow to the Heart. Pathology of Intrinsic Conductance System.

Exit
E N D
Presentation Transcript
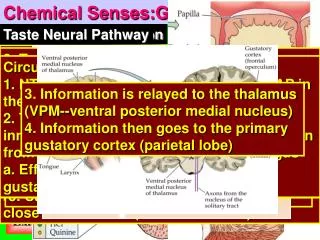
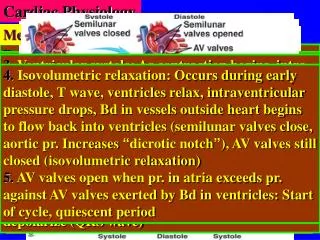
Cardiac Physiology Chambers of the Heart Anatomy of the heart Pathology Heart Physiology Blood Flow Through the Heart Mechanical Events during Heart Contraction Electrocardiography Heart Valves Cardiac Muscle Blood Flow to the Heart Pathology of Intrinsic Conductance System Extrinsic Control of the Heart Pericardium 1. Fibrous pericardium: Tense connective tissue, protects heart, anchors heart to surrounding tissues, prevents over filling 2. Serous pericardium: Parietal layer (Internal surface of fibrous pericardium), Visceral layer (epicardium: part of heart wall) 3. Pericardial cavity: Between serous layers, fluid filled to reduces friction between serous membr.s Myocardium: a. Cardiac muscle arranged in circular bundles b. Fibrous skeleton: Holds cardiac muscle together Endocardium: a. Inner myocardial surface b. Lines heart & connective tissues of valves c. Squamous epithelium Location: Within mediastinun of medial cavity of thorax, anterior to vertebral column, posterior to sternum, superior to diaphragm (at rest), superior margin (2nd rib), inferior margin (5th intercostal space), 60% of mass to the left of midline, base (posterior surface) faces right shoulder, apex points inferiorly toward left hip (contacts chest wall between 5th and 6th ribs & PMI-point of maximum intensity) E. Semilunar (SL) valves: Two: Aortic: Between left ventricle & aorta & pulmonary:Between right ventricle & pulmonary trunk. Open during ventr-icular contraction (systole): Intraventricular press-ure exceeds BP in aorta & pulmonary trunk. Three crescent shaped cusps open against arterial walls. F. No valves between atria & venae cavae & pulm-onary veins . Atrial contraction compresses venous entry points Heart requires its own circulatory system. Myocar-dium is too thick to permit diffusion. Coronary cir-culation: Arterial supply: Right & left coronary arteries (arise at base of aorta). Left: (supplies left side of heart by marginal branches: anterior inter-ventricular & circumflex arteries). Right: (supplies right side of heart: Marginal & posterior interven-tricular arteries). Anastomoses: Collateral routes of blood flow. Flow occurs only during diastole. 3. Ventricular systole: As contraction begins, intra-ventricular BP increase(AV valves close, semilunar valves closed),isovolumetric contraction phase“vol-ume constant” (BP in aorta&pulm. trunk exceeds intraventricular pressure, pr. in ven. increases without volume changing), ven. ejection phase (intraventr. pressure exceeds pressure in large vessels, semilunar valves open, Bd is propelled out of ventricles) & atria begin to fill with blood 3. Atrioventricular bundle (of His): Functional passage of impulse from atria to ventricles (no gap junctions between cells in atria & ventricles), Located in inferior interatrial septum, very short (branches to form bundle branches) 4. Bundle branches: Course interventricular septum toward apex of heart Two circuits: 1. Pulmonary: Right side of the heart a. Blood to lungs for gas exchange b. Right ventricle to left atrium of the heart c. Blood returns from body to right atrium, low O2 concentration, relatively high CO2 concentration d. Rt. Atrium to right ventricle e. Rt. Ventricle to lungs: Take O2 & give CO2, pulmonary arteries (away from heart, not CO2) f. Lungs to left atrium: Pulmonary veins, O2 rich Events: Na+ influx (slow) offset by K+ efflux (slow), K+ permeability gradually decreases, Influx of Na+ depolarizes cardiac cells, Depolarization opens fast Ca2+ channels, Ca2+ influx from ECS causes rising phase of AP, Repolarization increases K+ permeab-ility (cardiac cells repolarize), K+ channels inactivate, Cycle starts again Events 1. Start point: Atria & ventricles are relaxed (mid-to-late diastole) 2. Ventricular filling: Mid-to-late diastole, AV valves are open, semilunar valves are closed, vent-ricles begin to fill (70% occurs prior to atrial cont-raction), atrial systole (atria contract “preceded by P wave”, increased atrial pressure propels Bd from atria into ventricles), atria relax & ventricles depolarize (QRS wave) Characteristics 1. Branched, short, and interconnected fibers 2. Striated 3. Cardiac muscle fibers are functionally connected (intercalated discs, desmosomes, electrical coupling via gap junctions) 4. Functional syncytium: Entire myocardium acts as a single unit (result of gap junctions) Veins of right atrium: a. Superior vena cava: Return flow from regions superior to diaphragm b. Inferior vena cava: Return flow from regions inferior to diaphragm c. Coronary sinus: Drain blood from myocardium Layers of the heart 1. Three layers a. Epicardium b. Middle myocardium c. Deep endocardium 4. Isovolumetric relaxation: Occurs during early diastole, T wave, ventricles relax, intraventricular pressure drops, Bd in vessels outside heart begins to flow back into ventricles (semilunar valves close, aortic pr. Increases “dicrotic notch”), AV valves still closed (isovolumetric relaxation) 5. AV valves open when pr. in atria exceeds pr. against AV valves exerted by Bd in ventricles: Start of cycle, quiescent period 2. Systemic: left side of the heart a. Left atrium to left ventricle b. Left ventricle into aorta c. Aorta to body through systemic arteries: Gases and nutrients are exchanged d. Systemic veins to right atrium Ventricles: 1. Blood leaving the heart, 2. Most of mass of heart, right: anterior surface, left: inferior surface, 3. Muscles: Trabeculae carneae (cross-bars), papillary muscles (valve function, project into heart cavity), 4. Pulmonary trunk: Right ventricle, routes blood to lungs, 5. Aorta: Left ventricle, systemic circulation Four chambers: Two atria & two ventricles, heart is divided longitudinally: Interatrial & interventr-icular septa, atria receive returning blood (i.e., veins), auricles are appendages to increase atrial volume, fossa ovalis is residual impression of fetal foramen ovale 3. Work loads a. Equal volumes b. Unequal work loads c. Systemic: Five times as much resistance to blood flow, longer route d. Left ventricle is much larger & thicker to do more work C. Left AV valve:Bicuspid:Mitral valve:Two cusps D. Chordae tendineae (heart strings): Collagen cords attached to cusps, anchor cusps to papillary muscles during ventricular contraction, intraventr-icular pressure rises forces blood against valve flaps, chordae tendinea anchor flaps in closed postion A. Atrioventricular (AV) valves 1. Valves at atrium-ventricular junction 2. Prevent backflow into atria 3. Closed during ventricular contraction (systole) B. Right AV valve: tricuspid: Three cusps (reinforced endocardium) Cardiac veins: Follow course of coronary arteries, join to form coronary sinus to empty into right atrium. Tributaries: Great, middle & small cardiac veins. Anterior cardiac veins empty directly into right atrium. Angina pectoris: Temporary deficient blood flow to myocardium, thoracic pain is symptom Myocardial infarction (MI): Heart attack, Cardiac cells are amitotic, O2 deficiency causes necrosis (cell death), dead cells are replaced by noncontra-ctile scar tissue. Intrinsic conduction system: Noncontractile card-iac cells that initiate & distribute impulses from atria to ventricles. Autorhythmic, unstable RMP: Drift towards threshold. Pacemaker potentials: Membrane potential changes spontaneously Electrical changes during heart activity (ECG): Deflection waves 1. P wave: Depolarization moving from SA node through atria 2. QRS complex: Ventricular depolarization: Precedes contraction 3. T wave: Ventr. repolarization, occurs slower than depolarization: more spread out than QRS Intervals 1. P-R: Interval from beginning of atrial excitation &ventricular excitation, (includes: atrial depolariz-ation & contraction, passage of impulse through intrinsic conduction system), lasts 0.16 s 2. Q-T: Ventricular depolarization through repola-rization, includes: time of ventricular contraction 5. Purkinje fibers: Reach apex then branch super-iorly into ventricular walls, impulses in fibers moves faster than cell to cell contact (ensures greater pumping efficacy) Arrhythmias: Uncoordinated contractions B. Fibrillation: Rapid, irregular contractions Ectopic focus: Excitable tissue other than SA node controls heart contractions Heart block: Damage to AV node: Impulse cannot reach ventricles Location of autorhythmic cells 1. Sinoatrial (SA) node: Pacemaker: Fastest rate of depolarization, characteristic (sinus) rhythm. Located in right atrial wall, after depolarization is initiated, depolarization wave sweeps via gap junctions throughout atria Veins of left atrium Four pulmonary veins: Lungs back to heart, most of the posterior surface of the heart Cardiac cycle Systole (contraction) & diastole (relaxation), Length: Total 0.8 s, atrial systole 0.1 s, ventricular systole 0.3 s & quiescent period 0.4 s 2.Atrioventricular (AV) node: Depolarization wave initiated by SA node reaches AV node, AV node is located in interatrial septum near tricuspid valve, dia. of fibers is smaller (slows impulse conduction ‘0.1 s’ & permits completion of atrial contraction), impulse passes to bundle of His Brain-based control 1. Cardioaccelatory center in medulla, sympathetic NS control, innervate SA and AV nodes 2.Cardioinhibitory center, X nerve, parasympathe-tic system, innervate SA & AV nodes, slows HR Autorhythmic fibers: Pace maker cells: 1% of heart muscle, depolarize spontaneously Contractile muscle fibers: Depolarize in response to pacemaker cell activities Contraction 1. All cardiac muscle cells contract as a single unit 2. Self-excitable (i.e., autorhytmic): Initiate APs, independent of nervous innervation 3. Long refractory period: No tetanic contractions Home Exit BASIM ZWAIN LECTURE NOTES
Cardiac Physiology Heart Rate regulation Cardiac Output (CO) Heart Sounds Autonomic nervous system Factors that affect stroke volume 1. Preload-degree of stretch prior to contraction (most important +ve factor affecting EDV), factors increasing stretch: vol., speed of venous return & HR (time for filling) 2. Contractility: Increase in contractile strength ( independent of muscle stretch), increase Ca2+ into cardiac cells (increases contractility & vol. ejected from heart), decreased ESV, molecular regulation of contractile events Amount of Bd pumped by each ventricle per min.= Stroke volume X HR (SV= volume of Bd pumped out of each ventricle per beat). CO increase or decrease with SV or HR, .. SV= EDV- ESV EDV (end diastolic volume) is determined by length of ven. diastole & venous pr. (120 ml) ESV (end systolic volume) is determined by arterial pr. & Force of ven. contraction (50 ml) Associated with closing of heart valves: Lub-dupp- pause lub-dupp-pause, …Sound 1 (AV valves close, onset of systole, louder & longer than sound 2), sound 2 (semilunar valves close, beginning of vent-ricular diastole, short, sharp sound), pause (quiescent period). Sounds of separate valves can be differentiated: Timing (Mitral-Tricuspid-Aortic -Pulmonary) & location (four corners) 1. Sympathetic nervous system: Responds to real or perceived threats: Flight, fright, fight and sex 2. Sympathetic postganglionic neurons release NE at cardiac targets (mediated by ß1 adr. receptors: pacemaker cell RMP is brought closer to threshold ‘depolarized’ & increased HR) & increases Ca2+ influx into contractile cells (increases ESV) Chemical regulation: 1. Hormones: Adrenal medulla (Epinephrine ‘sym. NS’ increases HR and contractility ‘like NE’) 2. Ions: Ca2+ conc. (decrease causes depressed ht function & increase causes ht irritability Physical factors 1. Age: Inverse relation 2. Gender: Female faster 3. Exercise: Increased HR during exercise, resting rate is lower (bradycardia, SV & muscle mass increased in athlete) 4. Body temperature: HR lowered when cold 3. Parasympathetic division: Opposes sym. NS ( decreases HR), mediated by acetycholine (hyperpo-larizes ‘inhibits’ SA node) 4. Vagal tone: Sym. & parasym. divisions are continuously active (effect of parasym. division predominates) & dominant effect = reduce activity of AV node (25 beats/min reduction in HR) 3. Afterload-arterial BP: Pr. that ven. contraction must overcome (back pr. in aorta & pul. valves), normal: 80 mmHg (aorta) & 10 mmHg (pul. trunk) , not normally a factor in healthy individuals (may have an adverse effect in hypertensive subjects) CO is homeostatically regulated: Extrinsic factors induce change to cardiac function through: a. Neural mechanisms b. Chemical mechanisms c. Physical mechanisms Home Exit BASIM ZWAIN LECTURE NOTES