Download
1 / 23
230 likes | 407 Vues
FAME HTN. Mohsen. Epidemiology and stuff. About 1/3 of middle aged patients have hypertension About ½ of elderly patients have hypertension. Responsible for 12% of deaths worldwide. 5-6% reduction in diastolic blood pressure over 5 years reduces risk of CVA by 35-40% and IHD by 20-25%.

E N D
FAME HTN Mohsen
Epidemiology and stuff • About 1/3 of middle aged patients have hypertension • About ½ of elderly patients have hypertension. • Responsible for 12% of deaths worldwide. • 5-6% reduction in diastolic blood pressure over 5 years reduces risk of CVA by 35-40% and IHD by 20-25%
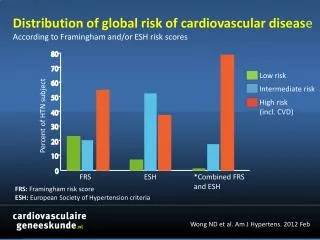
High blood pressure Tobacco High cholesterol Underweight Unsafe sex High BMI Physical inactivity High mortality, developing region Lower mortality, developing region Developed region Alcohol Indoor smoke from solid fuels Iron deficiency 0 1 2 3 4 5 6 7 8 Attributable Mortality (In millions; total 55,861,000) Proportion of deaths attributable to leading risk factors worldwide (2000)
Important Points: • Hypertension is the most common treatable risk factor for cardiovascular disease in patients over 50 ys. • Only 70% are aware they have HTN • Of those aware of their HTN, only 50% are being treated. • Only 25% of all hypertensive patients have their BP under control. • HTN is a risk factor for coronary artery disease (CAD), congestive heart failure (CHF), stroke, and renal failure.
Important Points: • For persons over age 50, SBP is a more important than DBP as CVD risk factor. • Persons who are normotensive at age 55 have a 90% lifetime risk for developing HTN. • Those with SBP 120–139 mmHg or DBP 80–89 mmHg should be considered prehypertensive who require health-promoting lifestyle modifications to prevent CVD.
ESSENTIAL HYPERTENSION • > 90% of all cases • multifactorial • interplay of genetics and environment • genes - polygenic • environment - obesity, salt, smoking • environment - intrauterine growth • MAJORITY OF CASES ASSOCIATED WITH HIGH CIRCULATING RENIN
Secondary hypertension • Coarctation of the aorta • Renal artery stenosis • Polyarteritis nodosa • Phaeochromocytoma • Conn’s syndrome • Polycystic kidney • Fibromuscular hyperplasia
Effects of Hypertension • Left ventricular hypertrophy • Coronary atheroma • Other atheroma (all medium/large blood vessels) • Acute myocardial infarction • Cerebral infarct • Cerebral haemorrhage • Hypertensive retinopathy • Renal impairment • Aortic dissection
Target Organ Damage Cerebrovascular disease - transient ischemic attacks - ischemic or hemorrhagic stroke Hypertensive retinopathy Left ventricular dysfunction/LVH Coronary artery disease - myocardial infarction - angina pectoris - congestive heart failure Chronic kidney disease Peripheral artery disease - intermittent claudication
Accurate BP Measurement • “Persons should be seated quietly for 5 minutes with feet on the floor and the arm supported at heart level” • Cuff must be appropriately sized (cuff bladder must encircle 80% of the arm) • Check both arms and a leg (or palpate pulses carefully) • Caffeine and Tobacco can transiently raise BP substantially
White Coat Hypertension • 20-30% of Apparently Resistant Hypertension May be due to “White-Coat Hypertension” • Patients with WCH have an increased risk of CV events and often have some degree of end organ damage • Use home or ambulatory monitoring to sort out
Home and Ambulatory BP Monitoring (ABPM) • Often lower than office readings • Useful to “calibrate” home monitors • Nocturnal Dip (10-20% fall during the night) is physiologically important (Dippers vs. Non-Dippers) • Can identify “windows of poor control” or windows of low BP and correlate with perceived symptoms
The assessment of the new hypertensive What do you do and why?
What to ask? • Height and weight. • Alcohol • Smoking • Diet, fats and salt • Exercise. • Stress.
Assess for secondary causes • When might you suspect this? • What might they be? • How would for check for them?
Other medical conditions to take into account. • Ischaemic heart disease. • Cerebrovascular disease. • Renal disease. • Peripheral vascular disease • Other conditions that might have a bearing on the treatment chosen.
Checking blood pressure at home • Some monitors are inaccurate and are not calibrated. • Wrist monitors are not usually accurate. • Can give multiple recordings and help in management of white coat hypertension. • Involves patient in the management. • Results should be factored up by 10/5.
White coat hypertension • Prevalence of 10-30% • Increases with age. • White coat hypertension maybe the precursor for hypertension. • There maybe an increased risk of CVD
Investigation of all patients with hypertension 1. Urinalysis 2. Complete blood count 3. Blood chemistry (potassium, sodium and creatinine) 4. Fasting glucose 5. Fasting total cholesterol and high density lipoprotein cholesterol (HDL), low density lipoprotein cholesterol (LDL), triglycerides 6. Standard 12-leads ECG Routine Laboratory Tests
Investigation for specific patient subgroups • For those with diabetes or renal disease: assess urinary protein excretion, since lower blood pressure targets are appropriate if proteinuria is present. • For those suspected of having an endocrine cause for the high blood pressure, or renovascular hypertension, see following slides. • Other secondary forms of hypertension require specific testing. Optional Laboratory Tests 1
Lifestyle Recommendations for Prevention of Hypertension for NON-Hypertensive Individuals. • To reduce the possibility of becoming hypertensive, • Healthy diet; High in fresh fruits, vegetables and low fat dairy products, low in saturated fat and salt in accordance with Canada's Guide to Healthy Eating • 2. Regular physical activity: accumulation of 30-60 minutes of moderate intensity dynamic exercise 3-5/week at least 4/week • 3. Low risk alcohol consumption (≤2 drinks/day or less than 14/week for men and less than 9/week for women) • Maintenance of ideal body weight (BMI 18.5-24.9 kg/m2) • Waist Circumference • < 102 cm for men • < 88 cm for women • 5. Restriction of salt intake to less than 100 mmol/day in individuals considered salt-sensitive, such as: Canadians of African descent, age over 45, individuals with impaired renal function or with diabetes. • Smoke free environment