Download
1 / 22
220 likes | 357 Vues
Safeguarding Adults and the NHS. Sylvia Manson. Introduction – Review of No Secrets. Our society is redefining how we enable adults to be safe from harm and abuse. No Secrets is being reviewed to provide a framework and principles that can guide local practice

E N D
Safeguarding Adults and the NHS Sylvia Manson
Introduction – Review of No Secrets • Our society is redefining how we enable adults to be safe from harm and abuse. • No Secrets is being reviewed to provide a framework and principles that can guide local practice • The NHS have a key role in safeguarding adults
Drivers for Change Safeguarding Adults Vision Safeguarding Adults Principles No Secrets 2 Specific Guidance
Primary Driver 1- Government Policy Shift power from state to local communities and individuals Big Society – greater involvement of voluntary agencies and communities; Maximise autonomy - limited state intervention Accountability to patients Democratic legitimacy Informed choice & control ‘no decision about me without me’ • Strengthened regulatory role • Break down barriers between Health and Social Care • Increased collaboration across statutory and 3rd sector • Decisions closer to people – GP consortia • Quality of care - Patient Safety • Quality Innovation Prevention & Productivity • Outcome focused AFFORDABILITY
Primary Driver 2 - Legislative Framework Existing Legislation Human Rights Act 1998 Mental Capacity Act 2005 amended 2007 NHS & Community Care Act 1990 Health and Social Care Act 2008 – regulation; direct payments Equalities Act 2010 Domestic Violence Crimes and Victims Act 2004 SVG Act ……… and the rest! Law Commission Review – April 2011 Social Care Bill – Autumn 2011
Case Law • Limitations of Local Authority duty and authority - to investigate, act where person lacks capacity, support, guide, inform and involve police where necessary Justice Hedley: Re Z (Local Authority: Duty (2004) EWHC 2817 (Fam). - to support not to control…. Court authority required before any attempt to control, coerceJustice Munby -A & C [2010] EWHC 978 (Fam) • Best Interest and Risk Enablement - sensible risk appraisal not striving to avoid all risk….. in particular to achieve the vital good of the elderly or vulnerable persons happiness. What good is making someone safer if it merely makes them miserable?’Justice Munby MM (An Adult) (2007) EWHC 2003 (Fam), (2009) • Use of Inherent Jurisdiction for those with Capacity - Capacitated persons ability and free choice to make decisions and give true consent may be impaired if under constraint, coersion, undue influence. Court may be asked to intervene but jurisdiction will be used sparingly and only to enable the person to make decisions without the external pressures Re SA (2005) EWHC 2942 (Fam)(Case related to forced marriage) – Justice Munby (JE 2009 unreported)
Primary Driver 3 – No Secrets Consultation People experiencing safeguarding reported They got lost in the system Safeguarding should not be at the cost of other qualities of life Wanted to be listened to & and to make choices They are not children General Prevention – pro active safeguarding system Balance protection and levels of intervention – enable people to take considered risk. The NHS Struggling to engage with safeguarding – seen as the LA responsibility Failure to recognise safeguarding concerns arise in NHS care Need to create culture of openness and learning Need for leadership and accountability Need to integrate clinical governance and safeguarding
Primary Driver 4 – Learning from Inquests, Inquiries & Research Steven Hoskins 2006- failures in identifying vulnerability & risk indicators; partnerships – information sharing; eligibility criteria; assessment of decision making capacity; Fiona Pilkington 2007 – failures in identifying vulnerability & risk indicators; failure to share information and refer on Margaret Panting 2001 – self determination balanced with duty of care • Mid Staffordshire – failures to focus on quality; failure to listen to patients; need for early warning systems; role of commissioners and regulators - failure to use intelligent information • Death by Indifference – institutional discrimination led to deaths • Cornwall Partnership NHS Trust 2006 inadequate arrangements to protect vulnerable adults; staff largely unaware of what constituted abuse. • Shipman Inquiry 2004; Kerr & Haslam 2005 • Etc Etc • AEA Prevalence Study 2007 • Womens Aid – Making the Links: Disabled Women and Domestic Violence 2008 • Domestic Abuse in older women; University of Sheffield ( Autumn 2010) • CSCI/HCC research – restrictive care; institutional abuse • Demographic Change – National Office Statistics
Distilling the Primary Drivers For Individuals Choice and control Enablement Full and informed consent Representation and making best interests decision for those lacking capacity. Least intrusive means • For Services and Systems • Focus on prevention • Limited intervention - proportionality • Partnerships and cooperation • Greater community involvement • Managing across plurality of providers and under new commissioning systems • Accountability for quality of services – to public , commissioners and regulators • Systems need to be affordable
We want people to be safe from harm and exploitation, and in control of their own lives
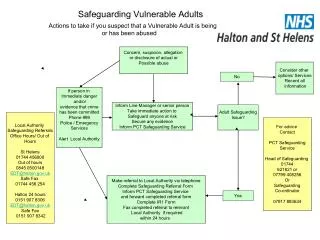
The NHS have a key role to play in their own services -preventing harm occurring and responding effectively where harm occurs The NHS also have a key role in supporting adults at risk within their own communities and within other services. What does this mean for the NHS?
Safeguarding is Integral to Quality & Outcomes Clinical Effectiveness Patient safety Dignity in Care Safeguarding Prevention Policy areas – E.G Dementia Strategy 6 Lives Carers strategy Patient Experience
Safeguarding as a continuum Safeguarding activity
Addressing Safeguarding – prevention and early intervention Patient empowerment • Build resilience factors – personal, social, environmental • Maximise decision making • Minimise the impact of disability/condition – Aids; adaptations; assistive technology; relapse prevention planning • Person centred planning - risk enablement ; ‘Stay safe’ personal plans • Effective communication - Information , choices • Promote advance planning – LPA; Advance decisions; statements of preference • Access to complaints • Patient involvement in service /strategic planning & review Prevention/early intervention in the care – ID higher risk patients – person centred care planning – support with eating drinking; Safe physical environments What are high risk areas of care? Pressure ulcer care? Discharge? ID risks in environment
Addressing Safeguarding – prevention and early intervention Care and Environment • Identify patients at greater risk of harm - e.g. assistance to eat and drink; pressure care; communication needs; enhanced discharge planning; privacy & dignity; consent; advocacy requirements? • How is use of restriction and restraint governed? • How are carers identified – carers assessments and support plans? • What are your organisations critical points of care? – e.g. Pressure ulcers; medication; discharge; capacity and capability of staff; managing challenging patient behaviours; • Which wards/services present highest risk? • How is clinical governance informing preventative/early intervention? • How do commissioners know that quality care is being delivered? • Strategic partnerships – Wellbeing and Health; Safer Communities Prevention/early intervention in the care – ID higher risk patients – person centred care planning – support with eating drinking; Safe physical environments What are high risk areas of care? Pressure ulcer care? Discharge? ID risks in environment
What is the patient’s desired outcome and how can they be supported to achieve this? Does the patient have capacity to make decisions about their safeguarding? – Maximise involvement; representation Who else may be at risk of harm? Who needs to be involved? Relationship with the patient Clinical/ specialist skills & knowledge required Roles & responsibilities required for investigation; risk assessment; support/protection plan & review Single agency or multi agency? How do we know we have improved the outcome for the patient? Addressing Safeguarding Concerns in Community Pathway
How are concerns identified and managed ? How are complaints and incidents integrated within safeguarding? How are decisions made about when to refer? How do you work with local multi agency safeguarding partners? - Cooperation Accountability Proportionality How are decisions made within your interagency procedures about internal or independent investigation? What’s the role of commissioners and regulators in this? How is the patient supported throughout? How do we know we have improved the outcome for the patient? How do we know lessons learned have improved outcomes? Addressing Safeguarding Concerns in Services
Clinical Governance & Safeguarding Serious case review - IMRs Serious Incident - reporting & investigation Safeguarding Procedures Preventative /Early Intervention Safeguarding Clinical incident –e.g. near miss