Download
1 / 42
670 likes | 2.34k Vues
Early Intervention in Psychosis. Presentation Outline. Terminology Child and Adolescent Onset Psychosis Early Intervention as a paradigm Recovery approach Psychopharmacology Early Intervention in ADHB and GPs. What is a psychosis?.

E N D
Presentation Outline • Terminology • Child and Adolescent Onset Psychosis • Early Intervention as a paradigm • Recovery approach • Psychopharmacology • Early Intervention in ADHB and GPs
What is a psychosis? • A severe mental disturbance indicating gross impairment in reality testing • Constellation of symptoms characterised by • Hallucinations • Delusions • Disorganisation of thoughts and behaviour.
Terminology • Psychosis occurs in a number of conditions • In practical terms working psychologically, the aetiological cause or basis of the psychosis is less relevant than the personal experience. • Psychosis and schizophrenia are ultimately medical terms to describe a constellation of experiences. • Medical terms such as ‘schizophrenia’ and ‘psychosis’ are questioned by some in terms of their validity and clinical usefulness
Schizophrenia • The striking heterogeneity of outcomes in schizophrenia challenges conventional notions of chronicity and therapeutic pessimism. • many long-term studies showing good long-term outcomes for schizophrenia [ up to 2/3 of subjects recovered or significantly improved over a 20 to 30 year duration ] • Changes of diagnosis frequent in first episode psychosis • Particularly in adolescents with 50% initial diagnosis changed • Usefulness of Psychosis NOS [avoid incorrect labelling / stigma]
Stress-vulnerability model • An episode of psychosis can be viewed as an interaction between • one or more environmental stressors; this may be physical [such as substance abuse or infection] or psychosocial [such as stressful life events or trauma] With • a vulnerability; vulnerabilities are factors that predispose someone to develop psychosis, but do not necessarily guarantee its development; examples include genetic or biochemical predisposition or previous injury or previous adverse negative life experience [sexual abuse]
Phases of Psychosis • Phase 1 – At Risk Mental State [formerly Prodrome] • early signs often non-specific, vague, insidious and unnoticeable and can resemble those of stress • changes in how people describe their feelings, thoughts, and perceptions • Sleep disturbance / depressed mood / social withdrawal / drop of in work study function / irritability / odd beliefs / odd behaviour • Phase 2 - Acute • clear psychotic symptoms i.e. hallucinations, delusions or confused thinking • Phase 3 - Recovery
Child and Adolescent Onset Psychosis • prevalence 0.9 in 10,000 at age 13; steady increase during adolescence; 17.6 in 10,000 at age 18 (Sweden) • Age-dependent variations in phenomenology • More insidious onset, more negative symptoms, greater disorganised behaviour, hallucinations in different modalities, fewer systematized or persecutory delusions
Child and Adolescent Onset Psychosis: Developmental Issues • Cognitive level of child influences ability to understand and express complex psychotic symptoms • Young children: True hallucinations vs. dreams; internal locus of hallucinations vs. inner speech/thoughts; formal thought disorder vs. immature language development; negative symptoms vs. anhedonia/depression • Developmental – bio – psycho – social – cultural model
Background and Origins • 1938: “Therapeutic results obtained in schizophrenia are considerably better in patients in whom there is little progression towards chronicity” (Cameron, USA) Nevertheless: • Kraepelinian view of schizophrenia as a relentless dementing illness associated with inevitable deterioration prevailed • Treatment approaches focussed on diagnosis, symptom management and chronic disease management
Origins – Early Psychosis Services • 1980s & early 90s: Studies confirmed prognostic influence of length of untreated psychosis on outcome • Early Intervention in Psychosis as a service model evolved in the mid 1980s • EPPIC in Melbourne • IRIS in Birmingham UK • Landed in NZ 15+ years ago
Why early detection and intervention • The loss of contact with reality that is characteristic of psychosis is a very frightening and traumatising experience. First episode particularly so. • first episode typically occurs in adolescence or early adulthood : a time that is important for the development of identity, independence, sexuality, relationships, study and career plans. • potentially causes significant disruption to these vital developmental tasks.
Early Intervention:A paradigm shift in Psychiatry • Change in paradigm: -From management and containment to recovery and prevention -Biological determinism to the stress-vulnerability model - Medical to bio-psychosocial and multi-disciplinary -Pessimism to optimism -Focus on diagnosis to symptom description -Pathologisation to normalisation - Individual focus to a wider systems based approach
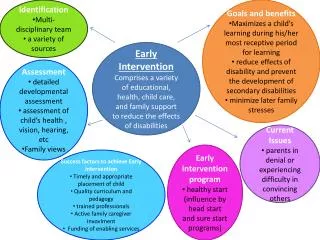
Aims of Early Intervention‘Prevent, Reduce, Preserve’ • Prevent interference with psychological and social development • Reduce delay between the onset of symptoms and access to treatment • Preserve relationships, prevent loss of social supports • Prevent unnecessary hospital admissions, reduce stress and trauma • Reduce secondary mental health difficulties eg; depression, substance abuse, anxiety • Preserve identity and hope
Aims of Early Interventioncont… • Reduce disruption to vocational and study roles • To ensure the individual and family are active participants in the recovery process ‘drivers not passengers’ • Raise community awareness • Improve prognosis and outcome
Principles of an EI approach • Early detection and treatment (reducing DUP, intensive input in ‘critical period’) • Reducing barriers to treatment • low threshold for assessment • Focus on engagement • Intensive inputs enabled by lower case loads • Developmentally responsive and youth focussed service • Family interventions • Optimistic recovery focus • Naturalistic supports • Least restrictive practice and environments • Appropriate risk taking • Assertive follow up • Assertive Outreach (and In-reach) approach
Principles of an EI approach cont… Symptoms rather than diagnosis “Its all psychosis” embrace diagnostic ambiguity Clients’ own words Increased emphasis on psychosocial treatments Relapse Prevention Collaborative approach Shared understanding and decision making Educative approach Flexible team based approach and flat team structure Mental Health Promotion Reducing stigma and delays to treatment Ongoing research and continuing education
Consequences of Delays • Increased hospital admissions • Increased cost of management • Delays in providing effective treatment for psychosis has significant effects outcome
Consequences of Delays • Interference with psychological and social development • Strain on relationships • family and peer • Increased disruption of study/employment • Substance abuse
Consequences of Delays • Slower and less complete recovery • Poorer longer-term prognosis • Increased risk of depression & suicide
High Risk Client Group First Episode Psychosis clients at high risk of: • Relapse (80% within 5 years) • Chronicity • Clinical morbidity • Disability (only 12% with psychosis are employed) • Social isolation and deprivation • Suicide • Emotional dysfunction • Co-morbidity (especially depression) • Psychological distress • Substance abuse • Iatrogenic trauma • Health issues (diabetes, cancer, CVD, respiratory illness) • Smoking (2x as likely to smoke)
Suicide • Suicide risk is a major consideration • Suicide attempt made by about 15% to 25% of first episode psychosis patients prior to treatment. • (?)10% of individuals with schizophrenia likely to complete suicide (5-13%) • of these 2/3 will do so in the first 6 years.
Potential Benefits of Early Intervention • Better prognosis • Preservation of psychosocial skills • Preservation of family and social supports • Decreased need for hospitalisation
Potential Benefits of Early Intervention • Reduce risk of relapse • Reduced morbidity • More rapid recovery
‘critical period’(Max Birchwood) • When disabilities develop during a first episode of psychosis they usually do so during the so-called critical period of the first 3-5 years. • A critical period for vulnerability to relapse, and development of secondary handicaps. • For example unemployment, impoverished social networks, and loss of self-esteem can develop during the critical period.
critical period’(Max Birchwood) • The longer these needs are not dealt with the more entrenched they become. • In this period the severity of the enduring psychotic condition is to be established.
duration of untreated psychosis • Delaying treatment causes a psychotic illness to become entrenched and less responsive to treatment. • A long duration of untreated psychosis [DUP] has been associated with slower and less complete recovery, and greater relapse rates. • There is frequently a considerable delay between the onset of symptoms and the commencement of appropriate treatment, on average 12 months. • Factors that contribute to this delay include societal stigma, poor recognition, variable patient insight.
Plateau effect • In contrast to Kraepelin’s concept of “dementia praecox”, schizophrenia is not necessarily a deteriorating and inevitably socially disabling disorder. • There is a plateau effect, in which if a deterioration does occur, it does so aggressively in the first 2-3 years.
Recovery • Psychiatric services have historically emphasised maintenance rather than recovery. • The recovery paradigm has become an increasingly vital component to working with individuals with significant mental health troubles.
Recovery • A process by which a person accepts that their life has been irrevocably changed and finds new opportunities to develop a satisfying and fulfilling life within their new circumstances. • Frequently described as “having a life worth living on my own terms and of my own choosing”. This is not the same as a “medical cure.”
Recovery • Informed choice is key. This may mean rejection of neuroleptic medications by some. • “We must have the opportunity to try and fail and to try again. In order to support the recovery process mental health professionals must not rob us of the opportunity to fail” • Patricia Deegan from “Recovery as a Journey of the Heart”
Recovery • An individual’s personal response to psychosis may impact on the recovery process. • For some people experiencing a first episode of psychosis, denial is adaptive where acceptance risks pessimism and despair. It may, however, come at the cost of non-adherence with treatment recommendations including in particular medications.
Recovery • Many EIS services utilise an approach of: • blame free acceptance of mental health troubles • with encouragement of a sense of mastery • through education, • teaching strategies to manage symptoms, • recognising and responding to early warning signs of relapse and • highlighting and challenging the stereotypes around psychotic experiences
Recovery • Other important recovery themes include • striving for meaning and purpose • self-responsibility • autonomy • sense of agency • having adequate and appropriate access to information to enable informed choices • self advocacy • provision of flexible support
Early Warning Signsrelapse prevention and relapse signature • “Relapse signature” refers to an individual’s idiosyncratic pattern of thoughts, feelings, behaviours and stressors that accompany a deterioration in mental health. • By exploring, documenting and monitoring for the early warning signs of this relapse signature, a relapse can be averted or at least ameliorated. • Easy to use, self-rating scales e.g. Early Warning Signs Scale for Psychosis
Psychopharmacology andEarly Intervention in Psychosis • The role of anti-psychotic medication in pre-psychotic states (prodrome/ARMS) remains controversial. • “Start low and go slow” using newer atypical antipsychotics • Aim for minimum effective dose • High vigilance and very low acceptance of side effects • Risperidone 2mg ; olanzapine 10mg ; quetiapine 300mg ; aripiprazole 15mg • Usually require far lower antipsychotic doses than established cases • Antipsychotic response may be several weeks; • First episode psychosis patients will benefit from a low stimulus environment. • Short term minor tranquilizers and psychological approaches will assist in regaining sleep patterns, reduce excess anxiety, agitation and panic.
Psychopharmacology cont.... • Heterogeneity of response in context of heterogeneity of diagnosis and aetiology • First episode psychosis of schizophrenia best clinical practice includes antipsychotic medication • titrating from very low doses, and using the minimum effective dosages. • medication should be continued for at least one year symptom free [higher risk of relapse in this period]. Then cautious reduction and stop • longer periods are recommended for those who show signs of relapse. • Less clear cut research evidence for psychosis due to other aetiologies but generally shorter periods for those likely to be suffering substance induced psychosis / brief psychotic episodes
EIT Services in ADHB • 5 teams: 4 adult and 1 adolescent • Multi-disciplinary (psychiatrists, psychologists, occupational therapists, social workers, nurses) • Well-resourced, small caseloads so more intensive input • Assertive outreach, flexibility in approach
What GPs can do- in the room with the client • Normalise the experiences (e.g. it’s common for people to hear voices at some time in their life, and particularly during heightened stress) • Validate distress • Take care with language – refer to symptoms/experiences rather than diagnosis • Hold hope • Introduce the client to the idea of working with an EI service
What GPs can do- making referrals to EIT services • Call us directly for an informal chat to gauge appropriateness of client for EI service • Referral through triage (as per standard process) • State in referral that EIT service is indicated • Continuing care/liaison • Aim is discharge back to GP care
Contact details for services • St Lukes CMHC 845-0940 • Manaaki House CMHC 570-6519 • Taylor Centre CMCH 376-1054 • Cornwall House CMHC 623-5780 • Kari Centre (youth) 623-4646 • Urgent after hours service: 0800 800 717
5 key points • People can and do recover from psychosis. Hope is important. • Be mindful of stigma. Take care with language. • We’re keen to talk with GPs, feel free to contact us with queries/concerns/curiosities • Pharmacology is not the only solution to psychosis – multidisciplinary teams • Early detection early intervention