Ventilator Associated Pneumonia
Ventilator Associated Pneumonia. Jeremy Fisher, PGY-3 VA vascular Surgery July 2011. 62M w / Systolic dysfn , HTN, DMII, smoking hx , POD 7 s/p Aorto -bi-fem bypass Kept intubated for pressor requirement post-op Now off pressors

Ventilator Associated Pneumonia
E N D
Presentation Transcript
Ventilator Associated Pneumonia Jeremy Fisher, PGY-3 VA vascular Surgery July 2011
62M w/ Systolic dysfn, HTN, DMII, smoking hx, POD 7 s/pAorto-bi-fem bypass Kept intubated for pressor requirement post-op Now off pressors Increased FiO2 from 0.40 to 0.50 o/n and increased PEEP 5->8 CXR w RML infiltrate and generalized haziness across both lung fields WBC 13.5 (11.0)
What is the diagnosis? Criteria? Further studies? Treatment? What could have prevented this?
Overview 1. Diagnosis 2. Incidence and Impact 3. Treatment 4. Prevention
Overview • Diagnosis What is VAP? Clinical Criteria Respiratory Sampling/Cx 2. Incidence and Impact 3. Treatment 4. Prevention
What is VAP? Pneumonia that develops in someone who has been intubated • Usually refers to those intubated >48 hours • Early onset <4 days • Late onset >4 days
Diagnosis of VAP • Clinical diagnosis is challenging and controversial • Suspect VAP when: • CXR – new or progressive infiltrate • AND • At least 2 of fever, abnormal WBC, purulent secretions • Obtain lower respiratory culture
Diagnosis of VAP • Clinical diagnosis is challenging and controversial • Suspect VAP when: • CXR – new or progressive infiltrate • AND • At least 2 of fever, abnormal WBC, purulent secretions • Obtain lower respiratory culture - Klompas, 2007 - Review/Meta analysis, - 14 Studies LR 1.7; 95% CI,1.1-2.5 LR 0.35; 95% CI,0.14-.87 LR, 2.8; 95% CI, 0.97-7.9 Incidence 9.7% then likelihood 23% Probability 3.6%
Diagnosis of VAP: CPIS Score CPIS > 6 Sensitivity 72-93% Specificity 42-85%
Diagnosis: Lower Respiratory Sampling Blind Bronchial Aspirate > 105CFUs • BronchoalveolarLavage • > 104CFUs Protected Brushings Mini–BAL
Diagnosis: Lower Respiratory Sampling If less than 50% of cells = Neutrophils VAP very unlikely (LR 0.05-0.10) Blind Bronchial Aspirate > 105CFUs • BronchoalveolarLavage • > 104CFUs Positive Gram Stain LR 2.1 for VAP Positive Gram Stain LR 18 for VAP Growth > 105CFUs LR 9.6 for VAP Growth > 104CFUs “Unhelpful”
Respiratory Sampling: Comparing the Methods • 90 Trauma patients with suspected VAP • BAL, blind aspirate, bronchoscopy brushings, blind brushings -Compared GS and Cx -Calculated agreement between modalities (kappa values) No statistically significant difference in yield
Diagnosis of VAP: Summary • Clinical diagnosis is challenging and controversial • Suspect VAP when: • CXR – new or progressive infiltrate • AND • At least 2 of fever, abnormal WBC, purulent secretions • Obtain lower respiratory culture • +GS more meaningful w/ deeper sample • +Cx >10,000 CFUs on BAL does not make diagnosis but may guide therapy (controversial) • >100,000 CFUs more convincing
Overview 1. Diagnosis 2. Incidence and Impact 3. Treatment 4. Prevention
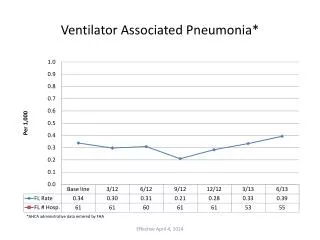
Incidence and Impact VAP occurs in 9-27% all intubated patients 2.1-10.7 episodes of VAP per 1000 ventilator days Barsanti, MC, Woeltje KF. “Infection Prevention in the Intensive Care Unit.” Infect DisClin N Am 23 (2009) 703–725. Apr 2009. Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J RespirCrit Care Med 2002;165(7):867–903.
Incidence and Impact Patients w VAP are twice as likely to die Significantly longer duration of ventilation and hospital stay Additional $10,000-40,000 Safdar N et al. Clinical and economic consequences of ventilator-associated pneumonia: a systematic review. Crit Care Med. 2005 Oct;33(10):2184-93
Overview 1. Diagnosis 2. Incidence and Impact 3. Treatment Bacteriology Strategy for Antibiosis Duration of Therapy 4. Prevention
Current Recommendations Infect DisClin N Am 23 (2009) 521–533
General Strategy Starting with broad spectrum antibiotic therapy improves mortality Choice of BS Abx regimen should be guided by institutional bacteriology Narrow coverage when possible (Cx guided) Double coverage for those at high risk for MDR
Duration of Therapy Reassess at 72 hours, narrow if possible, broaden if necessary Duration not well established in literature Some studies suggest 8 days is equivalent to 14 days (Chastre)
Overview 1. Diagnosis 2. Incidence and Impact 3. Treatment 4. Prevention
Prevention Evidence Driven Factors to Reduce VAP • High RN to Pt ratio • Reduced use of invasive ventilation • Semirecumbent positioning • Continuous aspiration of subglottic secretions • ET cuff pressure >20 cm H2O • Silver coated ET tubes Barsanti, MC, Woeltje KF. “Infection Prevention in the Intensive Care Unit.” Infect DisClin N Am 23 (2009) 703–725. Apr 2009.
Prevention Controversial Interventions • Slightly decreased rate of VAP w/ use of sucralfate in place of ranitidine, but increased risk of GIB (8 trials) • Oral care w/ chlorhexidine decreases VAP rates for those intubated <48hrs • Abx w/o diagnosis of VAP not recommended Barsanti, MC, Woeltje KF. “Infection Prevention in the Intensive Care Unit.” Infect DisClin N Am 23 (2009) 703–725. Apr 2009.
REMEMBER! 1.VAP is common and costly (in lives and $) 2. New/progressive infiltrate on CXR + 2 (fever, abnormal WBC, purulent secretions) -> high clinical suspicion for VAP 3. BS abx as guided by local bacteriology, double coverage for those at high risk for MDR (esp pseudomonas) 4. Good nursing w/ HOB elevated and suctioning can reduce rates of VAP