Download
1 / 17
170 likes | 335 Vues
Relationship of Early Physician Follow-up and 30-Day Readmission after NSTEMI Among Older Patients. Connie N. Hess, MD, Bimal R. Shah, MD, MBA, S. Andrew Peng, MS, Laine Thomas, PhD, Matthew T. Roe, MD, MHS, Eric D. Peterson, MD, MPH. Disclosures. C.N . Hess: None. S . Peng: None.

E N D
Relationship of Early Physician Follow-up and 30-Day Readmission after NSTEMI Among Older Patients Connie N. Hess, MD, Bimal R. Shah, MD, MBA, S. Andrew Peng, MS, Laine Thomas, PhD, Matthew T. Roe, MD, MHS, Eric D. Peterson, MD, MPH
Disclosures C.N. Hess: None. S. Peng: None. L. Thomas: None. M.T. Roe:Bristol Myers Squibb, Eli Lilly, Hoffmann-La Roche, Novartis. Astrazeneca, HelsinnPharmaceuticals, KAI Pharmaceuticals, Merck & Co., Sanofi-Aventis, Orexigen, Regeneron. B.R. Shah: None. E.D. Peterson:Eli Lilly, Janssen Pharmaceuticals.
Background • Strategies to reduce readmissions have focused on transitions of care processes. • Prior data suggest that early physician follow-up after hospitalization for heart failure may reduce readmissions.1 • Whether this strategy is effective for acute myocardial infarction (AMI) patients is unknown. 1Hernandez, AF et al. JAMA.2010;303:1716-1722
Objectives • To characterize hospital variation in early physician follow-up after discharge for non-ST-segment elevation myocardial infarction (NSTEMI) • To examine the relationship between rates of early physician follow-up and risk of readmission
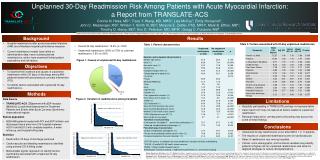
Methods: Data sources and study population NSTEMI pts ≥65 years surviving to hospital discharge (n= 42,568) • Clinical data from CRUSADE registry linked with longitudinal Medicare claims data from 2003-2006 • Transfer to acute care facility (n= 4,474) • Transfer to skilled nursing facility/hospice (n= 6,305) Patients discharged home (n= 31,789) • Non-index admissions (n= 949) • Hospitals w/o PCI & CABG (n= 3,849) • Hospitals with < 25 pts remaining (n= 927) Analysis population: n= 27,852 patients at 228 sites
Methods: Definitions and outcome • Early physician follow-up • MD visit within 7 days of discharge • Primary outcome: 30-day all-cause readmission
Methods: Statistical analyses • Logistic regression with hospital as random effect to examine hospital-level early follow-up and 30-day readmission • Adjustment models: 1) Patient demographic and clinical characteristics 2) #1 + hospital features (bed size, region, academic status) 3) #2 + treatment features (discharge medications, revascularization)
Variation in hospital-level early physician follow-up Number of hospitals Hospital early physician follow-up
Unadjusted 30-day readmission by hospital-level early physician follow-up p = 0.13 30-day readmission (%)
Adjusted 30-day readmission by hospital-level early physician follow-up Model 1 Quartile 2 Quartile 3 Quartile 4 Model 2 Quartile 2 Quartile 3 Quartile 4 Model 3 Quartile 2 Quartile 3 Quartile 4
Study limitations • Observational study - residual confounding • No data regarding non-physician post-discharge medical contacts • Limited to follow-up w/in 7 days and readmission w/in 30 days • Hospital-level measure insensitive • Low overall rates of early follow-up
Conclusions • 1 in 5 older NSTEMI patient readmitted within 30 days of discharge • Most patients not seen in follow-up by a physician within 7 days of discharge • Overall hospital rate of early physician follow-up low but variable • No association between early physician follow-up and 30-day readmission demonstrated
Future directions • Prospective assessment of early physician follow-up and readmission • Examination of other strategies to reduce readmission after AMI • Effectiveness of early follow-up as part of bundled strategy rather than isolated intervention