Download
1 / 49
560 likes | 914 Vues
Caries Risk Assessment and Clinical Care Paths. Norman Tinanoff University of Maryland August 3, 2011. History of Access to Care in Maryland. Develop a unified and culturally and linguistically appropriate oral health messages to educate parents and caregivers of young children

E N D
Caries Risk Assessment and Clinical Care Paths Norman Tinanoff University of Maryland August 3, 2011
Develop a unified and culturally and linguistically appropriate oral health messages to educate parents and caregivers of young children Incorporate dental screenings with vision and hearing screenings for public school children or require dental exams prior to school entry. Provide trainingto dental and medical providers to provide oral health risk assessments, educate parents/caregivers about oral health, and to assist families in establishing a dental home for all children. Initiate statewide single vendor dental Administrative Services Only provider Increase dental reimbursement rates to the 50th percentile Maintain and enhance the dental public health infrastructure by ensuring that local jurisdiction has a local health department dental clinic and a community oral health safety net clinic and by providing funding Establish a public health level dental hygienist to provide screenings, prophylaxis, fluoride varnish, sealants, and x-rays in public health settings. Dental Action Committee RecommendationsSept. 2007 (6 months after D. Driver died)
Dental Action Committee7 Recommendations • Increase dental reimbursement rates (indexed by inflation) to median fee charged by area dentists (ADA 50th percentile) – began July 1, 2008 • First of 3 annual increments – most diagnostic and all preventive rates increased • Single payer dental Medicaid program – carve out from Medicaid program • Implemented – July 2009 • Insurance company has to have a provider identified for every child • Increase the dental public health infrastructure - $2M/yr. • Funding to Office of Oral Health in July 2008 • Funding for local health department, federally qualified health center (FQHC) and private, & non-profit dental programs • New dental clinical programs in 6 Maryland counties previously without public health dental services
Dental Action Committee7 Recommendations • Expand the role of dental hygienists in public health practice • Legislation (HB 1280/SB 818) unanimously passed --October 2008 • Pediatric dental training of physicians and general dentists • Fluoride varnish initiatives - Medicaid reimbursement to physicians in July 2009 • 400 physicians trained at the University of Maryland Dental School • 20,000 fluoride varnish claims ($.5M) • Oral health screenings required for school entrance • Demonstration project funded for one county in 2011 • Legislation pending for next state legislative session • Develop a unified educational/social marketing program • Federal Earmark of $1.3M from Senator Mikulsky • Deamonte Driver Program of Oral Health Access - $1.1M
History of Access to Care in Maryland Because of the tremendous increase in the population 9X more preventive services and 8X more restorative services were delivered in 12 years. However, the costs have increased from 2.7M in 1997 to 71.4 M in 2008 (26X).
As Bob Russell said last night, “Is this tremendous increase in effort and cost actually reducing dental disease?” Perhaps the system is inefficient without -- • Caries Risk Assessment • Dental Caries Protocols (Care Paths)
Physicians Use of Risk Assessment (e.g. Heart Disease) JAMA 285: 2486, 2001
Early Studies of Risk Assessment in Dentistry Bohannan et al. A summary of the results of the National Preventive Dentistry Demonstration Program. Can Dent Assoc J 6: 435, 1985 Demers et al. A multivariate model to predict caries increment in Montreal children age 5 years. Comm Dent Health 9:373, 1992 Disney et al. The University of North Carolina caries risk assessment study. Comm Dent Oral Epidemiol 20:64, 1992 Thibodeau and O’Sullivan. Mutans streptococci and caries prevalence in preschool children. Comm Dent Oral Epidemiol21:288, 1993 Litt MD et al. Multidimensional Causal Model of Dental Caries Development in Low-Income Preschool Children. Public Health Reports 110: 607, 1995 Caries diagnosis and risk assessment. A review of preventive and strategies and management. JADA 126:1S, 1995
Recent Emphasis on Risk Assessment in Dentistry • Gives understanding of the disease factors for a patient • Individualizes and selects preventive recommendations • Individualizes treatment • Less treatment for low risk; more for those at high risk
History and Evidence • previous caries • mutans streptococci • income and education • visible plaque • diet • fatalism • mother’s taste perception • multiple risk factors
Relationship of initial caries pattern to caries incidence in 142, 3- to 4-year-old (at baseline) inner city children initial caries patterns Baseline dmfsyear 2 dmfs caries free pit and fissure maxillary anterior 0.0 1.4 3.0 5.9 5.0 10.1 Thibodeau and O’Sullivan. Comm Dent Oral Epidemiol 21:288, 1993
All dmfs is Not the Same Probably arrested lesions Probably active lesions
All White Spot Lesions are Not the Same Probably arrested lesions Probably active lesions
Evidence for mothers as the source of MS in their children There are 17 studies in this area between 1975 and 2006, with the mean of 70.4% of children with at least one identical strain.
Relationship of mutans streptococci levels to caries incidence in 148, 3- to 4-year-old (at baseline) inner city children MS range baseline dmfs year 2 dmfs low 0.2 1.2 moderate 1.4 3.1 high 3.4 7.9 Thibodeau and O’Sullivan. Comm Dent Oral Epidemiol 21:288, 1993
Microbial Indicators of Dental Caries in Children Under Three Years of Age Park et al. Caries Res 40:277, 2006
Caries Experience by Economic Situation in U.S. 2-5-Year-Old ChildrenNHANES III, 1988-1994
Correlation of caries prevalence to SES indicators in 1,539 4-year-old Arizona children Tang et al. Public Health Reports 112: 319, 1997.
Correlation of Plaque on Primary Teeth and Caries Risk Aluluusua, S. et al. Comm Dent Oral Epi. 22: 273-276, 1994 Sensitivity 83%, Specificity 92% Lee CL, et al. J. Pub Hlth Dentistry 68:57-60, 2008 Correlation between % MS and plaque regrowth, R = 0.34; p <.05
Dietary Factors % with ECC Sig Eats breakfast every day no 34.6% yes 22.5% 0.001 Stopped bottle by 12 months no 26.5% yes 20.5% 0.02 Nunn et al., J Dent Res 88:361-366-275, 2009
Dental Fatalism % with ECC Sig “Most children eventually develop dental cavities” yes 76.7% no 23.3% 0.02 Ismail, et al. J Dent Res 88:270-275, 2009
Mothers’ Taste Perception as a Risk Factor for their Children's Dental Caries
Mothers’ Taste Perception as a Risk Factor for their Children's Dental Caries
Mothers’ Taste Perception as a Risk Factor for their Children's Dental Caries
Multidimensional Causal Model of Dental Caries Development in Low-Income Preschool Children HISTORICALPRESENT FUTURE psychological factors baby bottle usage sucrose consumption race/ethnicity parent’s dental knowledge mutans strep. levels D CARIES CARIES (86% of caries predicted) Litt et al. Public Health Reports 110: 607, 1995
Evidence for Caries Risk Assessment • Dental Caries Protocols (Care Paths)
Newsweek, March 2, 2009 $1 Billion for Comparative-Effective Research – research on best practices and measures which ones are most cost-effective. Health care in the US is a marvel of technology, consumes 1/6 of nations wealth, without making us comparatively healthy.
Newsweek, March 9, 2009 Coronary by-pass surgery in Texas is 5X those in Colorado; Back surgery in Wyoming is 6X those in Hawaii The difference in how conditions are treated are due to medical culture not to medical science Conclusion – need to allow for individual differences; but also need standards.
Rate of Orthopedic Procedures in Medicare Population, 2003Each point represents 1 of 300 health regions Wyoming mean mean Hawaii Congressional Budget Office, Research on the Comparative Effectiveness of Medical Treatments, Dec. 2007
Newsweek, March 23, 2009 …..decision to pursue one treatment over another is based more on professional bias and patient’s misperceptions than it is on sound science …… treatments each come with their own cadre of devotees, and members of one camp often don’t communicate with members of another.
April 29, 2009 The Affordable Care Act contains $1.1 billion for Comparative Effectiveness Research. The aim is to compare the clinical outcomes, effectiveness, and appropriateness of services, that are used to prevent, diagnose, or treat diseases.
Example of a Caries Protocol for a 0-2 Year-Old * Need to consider fluoride levels in drinking water
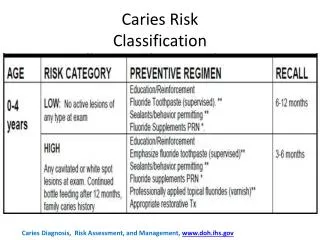
Active Surveillance (0-2 yr old) (prevention and careful monitoring for signs of progression) Low Caries Risk Toothbrush with F, .1% Toothbrush with F, .1% Professional F, 6 mo. Diet counseling Tests Caries Risk Analysis Clinical Exam Radiographic Exam Compliance Moderate Caries Risk Recall Toothbrush with F, .1% Professional F, 3 mo. Diet counseling Motivational Interview High Caries Risk
Example of a Caries Protocol for a 3-5 Year-Old * Need to consider fluoride levels in drinking water
Radiographic Criteria ADA & US Dept of Health and Human Services, 2004.
Topical Fluoride Hunter et al. Professionally Applied Topical Fluoride: Evidence-Based Clinical Recommendations. JADA 2006;137:1151-1159.
Example of a Caries Protocol for a >6 Year-Old * Need to consider fluoride levels in drinking water
Active Surveillance (>6 years old) Low Caries Risk Toothbrush with F, .1% Toothbrush with F, .1% Professional F, 6 mo. Sealants Xylitol Diet counseling Tests Caries Risk Analysis Clinical Exam Radiographic Exam Compliance Moderate Caries Risk Recall Toothbrush with F, .5% Professional F, 3 mo. Sealants Xylitol Diet counseling Motivational Interview High Caries Risk
June 14, 2011 Meeting • 17 experts from dental insurance, education and practice recommended guiding principles for the Pediatric Dental benefit of the Affordable Care Act to the Secretary of HHS: • Treatment should be based on individualized-care according to their level of disease • Treatment should be based on evidence-based guidelines