Download
1 / 40
400 likes | 1.28k Vues
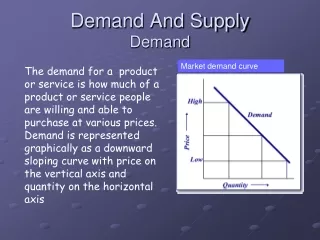
Supply and Demand of Physician Services. Econ 737.01. Supply and Demand of Physician Services: Outline. A. General Models B . Forms of Compensation C. Physician-Induced Demand. General Models: Outline. I. Supply of Physicians II. Supply of Physician Services

E N D
Supply and Demand of Physician Services Econ 737.01
Supply and Demand of Physician Services: Outline • A. General Models • B. Forms of Compensation • C. Physician-Induced Demand
General Models: Outline • I. Supply of Physicians • II. Supply of Physician Services • a. Model with Complete Information • b. Incomplete Information • c. Objectives Besides Income
I. Supply of Physicians • Summary Statistics (U.S.; 1994) • 126 medical schools • 16,000 graduates per year • 550,000 practicing physicians • 254 physicians per 100,000 residents • Average net income : $182,400 • Average work hours: 55/week • Physicians work a lot and make a lot • Market forces or shortage?
I. Supply of Physicians • Market distortions • Barriers to entry • Educational and licensing requirements • AMA controls these; incentive to restrict supply too much? • This would reduce supply below socially optimal level • Medical school subsidies • Could raise supply above socially optimal level
I. Supply of Physicians • Empirical Evidence • Difficult to measure physician shortages or excess returns on investments in medical education • 1900-1950 • Supply side: new medical school graduates constant • Demand side: average age, real per capita GDP, and insurance coverage all increased dramatically • Consistent with excessively restricted entry • More recently • Output of medical schools has expanded dramatically in last 10-20 years • Weeks et al. (1994): returns to education for physicians, lawyers, dentists, and MBAs all similar
II. Supply of Physician Servicesa. Model with Complete Information • Monopolistic Competition • Many sellers • Differentiated products (physicians are imperfect substitutes) • Some market power • Demand exogenous from physician’s perspective • Perfect information on both sides • Physicians maximize profit • Nonretradablegoods
II. Supply of Physician Servicesa. Model with Complete Information • Physician makes “all or nothing” offer to patient, who would prefer to consume less care at the given price • Physician can price discriminate • If price set by demand side (i.e. insurance companies/Medicare), physician responds by increasing quantity • Quality of service is another dimension to consider
II. Supply of Physician Servicesb. Incomplete Information • Punch line from part a: Even with perfect information, the differentiated and nonretradable nature of medical goods can keep medical expenditures above competitive levels. • Relaxing the assumption of perfect information further enhances our understanding of why medical expenditures are so high.
II. Supply of Physician Servicesb. Incomplete Information • 1) Irreducible uncertainty • Doctors and patients have imperfect information about the underlying condition and effectiveness of treatments • Most doctors and patients are risk averse • => increased test frequency and treatment intensity
II. Supply of Physician Servicesb. Incomplete Information • 2) Principal-agent problem • Principal: patient • Agent: doctor • Doctors know more than patients about appropriate level of care (asymmetric information) • Outcomes are often difficult for patient to observe • Often gray areas about appropriate treatment • => Could lead to excessive provision of care • “Induced demand”
II. Supply of Physician Servicesb. Incomplete Information • 3) Unobservable physician quality • Large fixed cost with trying a new physician • Information asymmetry makes it hard to observe physician quality • => Prices may not fully adjust to an increase in competition
II. Supply of Physician Servicesc. Objectives Besides Income • Parts a and b assume that physicians act to maximize income. Other considerations: • 1) Medical ethics: legal and moral constraints • 2) Patient’s best interest (patient’s utility enters into doctor’s utility function) • Patient’s utility, not society’s utility. Why is this an important distinction? • 3) Target income
II. Supply of Physician Servicesc. Objectives Besides Income • 3) Target income • Motivation: explain positive association between physicians per capita and prices of services, negative association between fees paid and quantity supplied • Physicians aim to maintain a “target income” • If increased competition lowers their income, they take advantage of their market power by raising prices or inducing demand to keep income relatively stable • What does this say about physician behavior before the increase in competition?
II. Supply of Physician Servicesc. Objectives Besides Income • 3) Target income • Taken seriously for a long time • Generally rejected now, though still subject of debate in literature • If target income hypothesis is true, there should be large income effects on supply (identified using non-labor income), and this doesn’t seem to be the case • Can you think of other explanations for the apparent paradoxes?
Forms of Compensation • I. Fee-for-service • II. Capitation • III. Salary • IV. Pay-for-performance
I. Fee-for-service • Physicians are paid an additional amount of money for each service they provide • Would expect this to increase the amount of care provided • Open question how much these additional services would improve health • Schuster et al. (1998) estimate up to 30% of services are not medically necessary • Often supplemented with incentives to economize
I. Fee-for-service • Who sets the fees? • Used to be physicians • In response to incentive problems, insurance plans began negotiating fees and Medicare began setting fees • These groups can do this because they are large enough that they have market power (monopsony) • How does this tie into the “public option” debate?
II. Capitation • Physicians receive fixed amount of money for providing services to a patient for a particular period of time • Incentive to keep long patient roster but give them each as little attention as possible • Could lead to higher referral rates • Various schemes to makes physicians share in financial risk • Still need to provide enough care to attract and retain patients • Incentive to select healthy patients (cream skimming; cherry picking) • Fee for a patient is “risk adjusted” based on expected utilization • This adjustment only accounts for 10% of variation • Often supplemented with incentives to ensure sufficient quality of care • Could be combined with ffs in a “mixed” system
II. Capitation • Quantity • Capitation seems to be effective in reducing quantity and expenditures (is this good?) • Stearns et al. (1992) • Group of WI employees enrolled in IPA • Change from ffs to capitation system where physicians shared in financial risk of hospitatlization and specialty costs • Increased primary care visits by 18% • Decreased specialist visits by 45%, hospital visits by 16%, and length of stay by 12%
II. Capitation • Quantity • Ogden et al. (1990) • Group of IL employees enrolled in IPA • Switched from ffs to capitation with shared financial risk • Specialist costs increased 2% compared to 12% the previous year • Hospital outpatient costs dropped 7% compared to increasing 12% the previous year • Little change in inpatient hospital utilization
II. Capitation • Quantity • Mooney (1994) • GPs in Copenhagen, Denmark switched from capitation to mixed capitation-ffs • Provision of services that provided extra fees increased dramatically • Decrease in referrals to specialists and hospitals
II. Capitation • Quality • Sorbero et al. (2003): patients 36% more likely to switch physicians under capitation than ffs • Shen et al. (2004): survey with hypothetical treatment decisions; physicians more “bothered” by their decisions under capitation than ffs
II. Capitation • Referral rate • Capitation does seem to lead to more referrals on the margin, both theoretically and empirically, if the GP does not share in the financial risk • Theoretical: Barros and Martinez-Giralt (2003); Iverson and Luras (2000b) • Empirical: Forrest et al. (2003); Carlsen and Norheim (2003)
III. Salary • Provides fixed income to physician over a particular time period • Ex. in US: Staff HMOs • Incentive to do as little as possible to keep job • Often supplemented with incentives to ensure reasonable quantity and quality of care • Less common than others, but do see it in national health systems like UK and staff HMOs in US
IV. Pay-for-performance • Ties part of physician or hospital reimbursement to meeting performance thresholds (clinical outcomes, patient satisfaction, etc.) • New and largely untested • >20 million in US covered (Rosenthal et al., 2004) • Difficult to measure “performance” • What incentive problems might result from paying on the basis of outcomes?
Physician-Induced Demand • I. Theory • II. Evidence from Increased Competition • III. Evidence from Decreased Fees • IV. Summary
I. Theory • Physician-induced demand (PIP): “when the physician influences a patient’s demand for care against the physician’s interpretation of the best interest of the patient” (Handbook, p. 504) • Physician exploits role as agent to alter the patient’s demand curve • Distinctions that make PID challenging to identify empirically (not enough to just look at quantity) • Useful agency v. inducement • Demand shifting v. quantity setting
I. Theory • Model • Where Y=income, I=inducement, N=number of patients, m=margin, x=quantity, i=inducement • Solving yields
I. Theory • Testable prediction 1 • N down => Y down and I down => UI less negative and UY up => -UI/UY down => x1’ and x2’ down => i1 and i2 up. • So, increased competition for patients should increase the per-patient quantity of services • Supply side: more physicians in market • Demand side: less need for services • Depends on changing tradeoff between I and Y as income changes (income effect)
I. Theory • Testable prediction 2 • m1 down => UY up => -UI/UY down => i1 and i2 up • Income effect • m1 down => lower return to inducement in sector 1 => i1 down and i2 up • Substitution effect • Net effect on i1 ambiguous; net effect on i2 down • So, a drop in fees from one payer should increase quantity among patients with another payer
II. Evidence from Increased Competition • Effect of increase in per capita number of physicians on quantity • Problems • Really tests joint hypothesis of induced demand and income effects • Endogeneity of number of physicians (likely a response to demand)
II. Evidence from Increased Competition • Fuchs (1978) • Effect of supply of surgeons on surgeries • 22 metropolitan areas, pooled cross sections from 1963 and 1970 • IVs: metro area, hotel receipts, percent white • 10% increase in surgeons => 3% increase in surgeries • Cromwell and Mitchell (1986) • More years, more areas, better controls • Same identification strategy • Same sign, smaller effect • Birch (1988) and Grytten el at. (1990) • More dentists per capita => more dental visits
II. Evidence from Increased Competition • Rossiter and Wilensky (1983, 1984); Scott and Shell (1997) • Small effects of physician density on quantity for some procedures • Dranove and Wehner (1994) • Falsification test: estimated “effect” of number of obstetricians on volume of births • Similar IV methodology to Fuchs and Cromwell and Mitchell • Found positive effect; suggests methodology is suspect
II. Evidence from Increased Competition • Gruber and Owings (1996) • 13.5% fall in fertility from 1970-1982 represents exogenous shock to incomes of OB/GYNs • Exploited between-state over-time variation in fertility rates to identify effect on Caesarian section deliveries (more lucrative) • 10% drop in fertility => 0.6% increase in P(C-section)
II. Evidence from Increased Competition • Pauly (1980) • Used large individual-level dataset • Least informed patients should be the most susceptible to demand inducement • Poor patients in big cities should be the least informed • Found (small) effect of number of physicians on quantity of ambulatory care for this group
III. Evidence from Decreased Fees • Hadley and Lee (1978); Mitchell et al (1989) • Medicare price freezes during 1970s and 1980s led to increased utilization • Hurley et al. (1990); Hurley and Labelle (1995); Escarce (1993b) • No clear evidence of effect of own-fee changes on utilization • Not surprising; theoretical prediction ambiguous • Rochaix (1993) • GPs in Quebec changed mix of services in response to lowering of fees
III. Evidence from Decreased Fees • Rice (1983) • 1977: Medicare began setting fees in Colorado based on state-wide averages • Reduced fees in Denver-Boulder area; increased them in other areas • Physicians facing declining rates increased provision of surgery, medical services, and tests
III. Evidence from Decreased Fees • Nguyen and Derrick (1997) • Impact of Medicare fee reductions for “overpriced procedures” • For 20% of physicians who experienced the largest price reductions, 1% reduction in price => 0.4% increase in volume. • Yip (1998) • Reductions in Medicare fees for thoracic surgeons led to large increases in volume • Surgeons recouped 70% of lost income
IV. Summary • There is no perfect test for demand inducement, but theory generates predictions that lead to tests that are suggestive. • “It appears that, in response to economic considerations … physicians can induce demand for their services, they sometimes do induce demand, but that such responses are nether automatic nor unrestrained” (Elgar p. 265, citing Hurley and Lebelle, 1995).