Download
1 / 22
240 likes | 404 Vues
Martial Hamon, MD, FESC University Hospital of Caen Normandy, France. Are Benefits of Fondaparinux Maintained According to Various Procedural Strategies? Insights from OASIS 5. Prognostic Impact of Major Bleeding in Patients With Acute Coronary Syndromes.

E N D
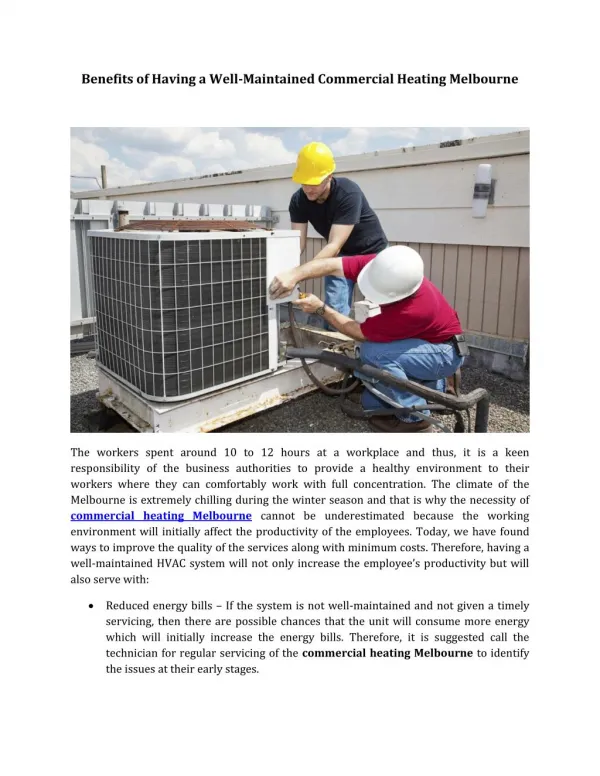
Martial Hamon, MD, FESC University Hospital of Caen Normandy, France Are Benefits of Fondaparinux Maintained According to Various Procedural Strategies? Insights from OASIS 5
Prognostic Impact of Major Bleeding in Patients With Acute Coronary Syndromes Pooled Relative Risks of Mortality Increase* Random-effects Meta-analysis of 10 Studies No Major Bleeding Major Bleeding Random Effects Model Study RR (95% CI) Deaths. No. / Patients. No. Ali et al 2004 9/89 24/931 3.92 [1.88. 8.18] Eikelboom et al 2006 60/470 833/33676 5.16 [4.04. 6.60] Feit et al 2007 10/194 9/5807 33.26 [13.67. 80.92] Kinnaird et al 2003 44/588 54/8992 12.46 [8.44. 18.39] Lenderink et al 2004 18/98 120/7702 11.79 [7.49. 18.55] Manoukian et al 2007 47/644 159/13175 6.05 [4.41. 8.29] Moscucci et al 2003 85/546 624/15348 3.83 [3.10. 4.72] Rao et al 2005 79/307 549/19110 8.96 [7.28. 11.02] Segev et al 2005 15/79 86/5763 12.72 [7.71. 21.01] Yusuf et al 2006 83/629 545/19449 4.71 [3.79. 5.85] Total (95% CI) 450/3644 3003/129953 7.60 [5.55. 10.40] Test for overall effect: Z = 12.65 (P < 0.00001) 0.01 0.1 1 10 100 N=133.597 patients Major Bleeding 2.7% Lower Mortality Higher Mortality RR (95% CI) (*in hospital or 30-Day) Hamon M. et al. EuroIntervention 2007 A Systematic Review and Meta-analysis
Entry site complications: Radial vs Femoral Meta-analysis of randomized studies Pooled Relative Risks of Access site complications Decrease* Random-effects Meta-analysis of 17 Studies Study Radial Femoral RR (random) RR (random) n/N n/N 95% CI 95% CI ACCESS 0/300 6/300 0.08 [0.00. 1.36] Achembach 0/152 4/155 0.11 [0.01. 2.09] BRAFE Stent 1/56 3/56 0.33 [0.04. 3.11] CARAFE 0/140 2/70 0.10 [0.00. 2.07] FARMI 2/57 11/57 0.18 [0.04. 0.78] Gorge 1/214 1/216 1.01 [0.06. 16.03] Grinfeld 0/138 3/141 0.15 [0.01. 2.80] Mann 1996 0/76 4/76 0.11 [0.01. 2.03] Mann 1998 0/74 3/68 0.13 [0.01. 2.50] Moriyama 0/108 3/92 0.12 [0.01. 2.33] OCTOPLUS 3/192 12/185 0.24 [0.07. 0.84] OUTCLAS 0/322 1/322 0.33 [0.01. 8.15] RADIAL-AMI 1/25 1/25 1.00 [0.07. 15.12] RADIAMI 0/50 3/50 0.14 [0.01. 2.70] Reddy 0/25 1/50 0.65 [0.03. 15.50] TEMPURA 0/77 2/72 0.19 [0.01. 3.83] Tian 0/189 2/195 0.21 [0.01. 4.27] Total (95% CI) 8/2195 62/2130 0.22 [0.12. 0.39] Test for overall effect: Z = 5.09 (P < 0.00001) Incidence: 0.36% vs 2.9% RR 0.22 [0.12-0.39]. 78% reduction NNT 39 0.001 0.01 0.1 1 10 100 1000 Favours Radial Favours Femoral Adapted and updated from Agostoni et al J Am Coll Cardiol 2004
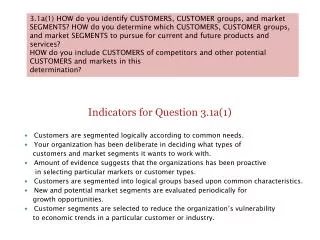
PCI Population in Oasis 5 during treatment period (Access sub-study analysis) • Impact of TRI on efficacy and bleeding in ACS patients • treated with a contemporary pharmacological regimen? 5565 PCI patients* 4971 Femoral access 594 Radial access 2519 Fondaparinux 2452 Enoxaparin 319 Fondaparinux 275Enoxaparin Post hoc analysis to examine the impact of the TRA vs TFA on PCI-related: major bleeding andpatients’outcomes *Patients randomized and that got treatment up to discharge or up to 8 days * Patients with deferred PCI,brachial access or whose records lacked access-site information excluded
Baseline Clinical Characterstics TFA 89% and TRA 11% 75 % 80 . 0 % 70 % Femoral = 4971 70 . 0 % Radial = 594 60 . 0 % 50 . 0 % 40 . 0 % 24 % 30 . 0 % 22 % 20 % 17 % 17 % 15 % 20 . 0 % 9 % 7 % 7 % 4 % 10 . 0 % 0 . 0 % Male* Diabetes* Heart Failure Prior MI* Prior PCI Prior CABG* *p<0.05
Similar High-risk Features in both Femoral and Radial access groups 71.9% 80 % 68.1% 70 % 60 % 43.8% 41.6% 50 % 40 % 30 % Troponin Positive ST Depression > 1mm 20 % 10 % 0 % Femoral Radial
Treatment Recommendations1 and Oasis 5 PCI Patients • ESC Guidelines for the management of NSTEACS Eur Heart J 2007;28:1598-1660 • [P<0.05 for ACEI and GPI]
High revascularization success rate whatever the vascular access 7944 lesions 7095 with femoral access 849 with radial access 3585 under Fondaparinux 3510 under Enoxaparin 460 under Fondaparinux 389 under Enoxaparin 92.1% 91.7% 93.7% 94.6%
Femoral = 7095 Radial = 849 Procedural DetailsStenting by Access site Percutaneous coronary interventions (analysis per lesion) 92.9% 91.6% 1.00 0.90 70.5% 70.7% 0.80 0.70 0.60 0.50 30.0% 0.40 25.4% 0.30 0.20 8.4% 7.1% 0.10 0.00 Any stent Bare stent Drug Eluting Stent* No *P<0.05
Most PCI’s performed within 72 hours At day 3: 75% in femoral group At day 3: 71% in radial group % PCI per day
Endpoint Measures at Day 9 Radial vs. Femoral Endpoint Femoral (n=4971) Hazard ratio ±95% CI Radial (n=594) p-value HR (95% CI) Net clinical outcome 8.6% 11.4% 0.74 (0.56-0.99) 0.043 Death/MI/RI 0.649 7.9% 8.5% 0.93 (0.69-1.26) Major bleeding 1.0% 3.7% 0.27 (0.12-0.62) 0.002 0 1 2 Radial better Femoral better
Endpoint Measures at Day 30 Radial vs. Femoral Endpoint HR (95% CI) Femoral (n=4971) Hazard ratio ±95% CI Radial (n=594) p-value Net clinical outcome 9.1% 12.8% 0.70 (0.53-0.93) 0.013 Death/MI/RI 0.399 8.4% 9.5% 0.88 (0.66-1.18) Major bleeding 1.2% 4.1% 0.28 (0.13-0.60) <0.001 0 1 2 Radial better Femoral better
Endpoint Measures at 6 months Radialvs.Femoral Endpoint HR (95% CI) Femoral (n=4971) Hazard ratio ±95% CI Radial (n=594) p-value Net clinical outcome 11.1% 15.9% 0.69 (0.53-0.88) 0.003 Death/MI/RI 0.14 10.1% 12.3% 0.82 (0.63-1.07) Major bleeding 1.5% 4.8% 0.31 (0.16-0.61) <0.001 0 1 2 Radial better Femoral better
Endpoint Measures: Radial vs Femoral Death, MI, RI Femoral Radial Death, MI, RI* 14% 12.3% 12% 10.1% 9.5% 10% 8.5% 8.4% 7.9% 8% 6% 4% 2% 0% day 9 day 30 day 180 *Primary endpoint of the study
Femoral Radial Mortality at 6 Months Radial vs. Femoral 3.4% 0.03 2.4% 0.02 Cumulative Hazard HR 0.68 95% CI [0.43-1.07] p=0.09 0.01 Non-adjusted: HR 0.68 [0.40-1.18] p=0.17 NNT~100 0.0 0 30 60 90 120 150 180 Days
Primary endpoint: Death, MI, RIin PCI patients at Day 9 (during blind study drug administration) P = 0.77 P = 0.47 HR 1.08 95% CI [0.62-1.89] HR 1.07 95% CI [0.89-1.30] 8.2% 8.8% 8.0% 7.8% (N=275) (N=319) (N=2452) (N=2519)
Protocol Major Bleedingin PCI patients at Day 9 (during blind study drug administration) P = 0.85 P <0.001 HR 0.86 95% CI [0.17- 4.26] HR 0.44 95% CI [0.32- 0.60] 5.1% 2.3% 1.1% 0.9% (N=275) (N=319) (N=2452) (N=2519)
GPI’s use in PCI patientsEndpoints Measures at day 9during blind study drug administration 5595 patients GPI + 2397 (43%) GPI- 3198 (57%) 1173 Enoxaparin 1224 Fondaparinux 1568 Enoxaparin 1630 Fonaparinux Enoxaparin Fondaparinux Major Bleeding HR 0.51 (95% CI, 0.34-0.78) Major Bleeding HR 0.37 (95% CI, 0.24-0.58) GPI+ GPI- P=0.002 p=<0.001
GPI’s use in PCI patientsEndpoints Measures at day 9Comparing Radial vs Femoral 5565 patients GPI + 2389 (43%) GPI- 3176 (57%) 2057 femoral 332 Radial 2914 Femoral 262 Radial Femoral Radial GPI+ GPI- P=0.08 P=0.08 P=0.02 P=0.03
ConclusionsInsights from OASIS 5 • Most PCI’s in NSTE-ACS patients are currently performed within 72 hours of admission by trans-femoral approach (TFA). • Compared to TFA, TRAis associated with similar rates of ischemia and significant reduction of major bleeding, leading to better net clinical outcome. • Wether TRA by reducing major bleeding can impact event-free survival warrants a randomized trial adequately powered. OASIS 5 access sub-study: post’hoc analysis (non randomised), hypothesis-generating analysis rather than hypothesis-testing. • A fondaparinux strategy: - Provides similar rates of ischemia compared to Enoxaparin either by TRA or TFA - Reduces major bleeding and Improves net clinical outcome in TFA compared to an enoxaparin based regimen with or without GPI. Modifiable factors : Arterial access site & Antithrombotic regimen
Identification of Risk Factors For Bleeding in ACS Patients and Preventive actions Identification Prevention Hamon M. et al. EuroIntervention 2007