Download
1 / 33
350 likes | 595 Vues
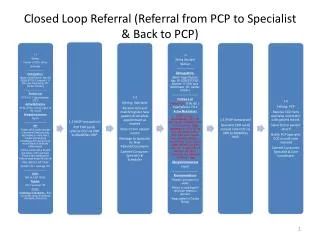
Referral from GPs to specialists. Why do GPs refer patients to specialists?. General reasons for referral by GPs to specialists. To establish the diagnosis For specific investigations (not available in the community) For specific treatment or operation For advice on management

E N D
General reasons for referral by GPs to specialists • To establish the diagnosis • For specific investigations (not available in the community) • For specific treatment or operation • For advice on management • For specialist to take over management • To reassure the GP • To reassure the patient/ relatives
Distribution of reasons for referral • Diagnosis 28% • Special investigation 7% • Specific treatment or op. 35% • Advice on management 14% • Specialist management 9% • Reassure GP 2% • Reassure patient/ family 2% • Other 2%
Issues to consider in defining referral criteria • Diagnosis • Special tests – fundoscopy • Development of complications • Neuropathy • Renal disease • Retinopathy treatment • Poor control • Commencement of insulin therapy??
Consider reasons for referral to a specialist in respect of specific chronic diseases Devise referral criteria for each chronic disease
Dangers of inappropriate or excessive referral • Incorrect labelling • Collusion of anonymity (Balint M. The Doctor, his Patient and the Illness) • Somatic fixation • Deskilling of the GP • Deskilling of the specialist
Dangers of insufficient referrals • Deprive patients of benefits of high-tech medicine • Deterioration of patient’s condition - perhaps to point where treatment becomes • more hazardous • less beneficial • futile • Lose touch with medical developments
What is an appropriate referral? • Appropriate to whom • specialist • GP • patient • What will be gained • health gain • prevention of health loss • social gain
Advantages of the GP gatekeeper system – for GPs • it enables them to keep track of all the patient’s problems and to be kept abreast of the patients conditions and their diagnosis and treatment. • it is more satisfying for the GP to hold onto patients he or she can manage themselves • it is a stimulus to continuing professional development
Advantages of the GP gatekeeper system – for specialists • it allows them to maintain their special skills without having these diluted by dealing with larger numbers of people with little or no illness. • it ensures that his or her skills are used to best effect • it avoids the specialist having to deal with other problems where he or she may be lacking expertise
Advantages of the GP gatekeeper system – for patients • it avoids the patient having to judge his or her own condition and decide if it requires a specialist • it avoids having to choose which specialist to attend • it avoids the risks attendant on getting either of these decisions wrong • it may avoid undue expense (specialists generally charge more than generalists regardless of the nature of the problem ultimately diagnosed.
Advantages of the GP gatekeeper system – for the healthcare system • it should lead to the most effective use of resources – both specialist and GP • it certainly helps contain healthcare costs • it can lead to better health outcomes overall
Disadvantages of the GP gatekeeper system – for GPs • it places all the responsibility for the referral decisions on him or her • it may lead to him or her coming under pressure from the health payment system to restrict access to expensive specialist • it may lead to pressure from patients to refer to specialists that the GP does not see as appropriate.
Disadvantages of the GP gatekeeper system – for specialists • it may mean that patients whom he/she would like to see, possibly at an early stage of their illness may not be seen because they have not made it past the GP gatekeeper • it may be seen by some specialists as a restriction on their practice (or earning capacity)
Disadvantages of the GP gatekeeper system – for patients • it can also be perceived as a restriction on their choice of healthcare provision • it can lead to worse outcomes if the gate is too restrictive
Disadvantages of the GP gatekeeper system – for the healthcare system • it can negate the usual effects of market forces (and so both specialists and GPs may be able to charge the system more for their services • it can be more difficult to administer • it may be unpopular with patients which will make it politically unattractive to a democratically elected administration
Contents of the referral letter - I (ideal) • Name, address, dob(age) of patient • Presenting complaint/ problem • History of presenting complaint • Past medical history • Current (& ? Past) medication(s) • Allergies (if any) • Social history (relevant - esp. carers)
Contents of the referral letter - II (ideal) • Findings on examination • Results of any investigations • Your opinion of problem/ diagnosis • Reason for referral • Any specific information/ service needed from specialist
Contents of the discharge letter (ideal) • Summary of symptoms • Examination findings • Results of investigations • Diagnosis or summary of problem(s) • Management plan • Nature and quantity of drugs issued • Information given to patient and/or relatives • Follow up arrangements • Advice of future management
Performance review • Referred patients an easily identifiable and important group • Cohort or case based review(s) possible • ? Interface audit - primary & secondary care • Referral criteria • Referral standards
Alternatives to referral • Telephone consultation • Domiciliary visit • Specialist outreach e.g liaison psychiatry • Joint consultation • Tele-medicine