Download
1 / 39
400 likes | 435 Vues
Learn about the importance, physiology, and assessment of nutrition in surgical patients. Explore the aetiology and pathophysiology of malnutrition, along with treatment principles and nutritional rehabilitation methods for optimal recovery. Stay informed on current trends and future directions in surgical nutrition.

E N D
NUTRITION IN SURGERY DR IBRAHIM S.S DEPT OF ORTHOPAEDICS JUTH
Outline • Introduction • Statement of surgical importance • Physiology of nutrition • Aetiology of malnutrition • Pathophysiology of malnutrition • Assessment of nutritional status
Outline (cont’d) • Classification of malnutrition • Principles of treatment of malnutrition • Methods of nutritional rehabilitation • Current trends • Future trend • conclusion
introduction • Malnutrition is common • It is frequently unrecognized and patients often do not receive appropriate support • Patients at risk have to be identified and be nutritionaly supported by the most appropriate route
INTRODUTION Nutrition – The process of utilizing exogenous substances for the production of energy and the synthesis of new tissues. Food – Any substance that can be used by the body to produce energy or some essential nutrients. Malnutrition is recognized as an important factor affecting the outcome of many surgical patients.
Introduction (cont’d) • John Hunter (1790)- Described use of tube enteral feeding • Dudrick & colleagues (1968)- Demonstrated the first successful use of TPN
Christopher Wren: infuse morphine to a dog – oleic acid to a horse. • Later; infusion of alcohol and milk. • Henriques and Anderson; hydrolysed casein to a goat. • 1936- Robert Ellman: first successful adm. of protein hydrolysate to human. • 1944- Helfrick and Abelson: intact support with iv fat and protein.
Statement of surgical importance • Over 50% of surgical patients have nutritional disorders • Nutritional status deteriorates during hospital stay • Increase Morbidity and mortality correlates with malnutrition • adequate nutrition is essential in surgical practice
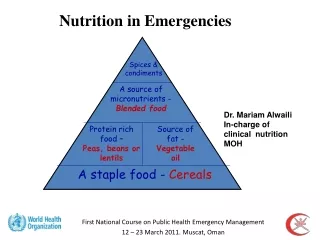
physiology of nutrition • Requirement varies with age,sex,metabolic activity • Daily requirement is such that; CHO(50%), Fats(35%), Proteins(15%) • Substances incorporated in synthesis of tissues; Prots, vits, trace elements, water & elecrolytes
Nutrients and their daily requirements Basal requirements: Adults/Kg • Energy: 125-146 joules • Carbohydrates: 4.2-6.0g • Protein: 0.7-1.0g • Fat: 1.5-2.0g • Water: 45-50ml (Tropics)
Nutrients and their daily requirements Basal requirements: Neonates/Infants/Kg • Energy: 377-502 joules • Carbohydrates: 12-18g • Protein: 2.5g • Fat: 4.0g • Water: 125-150ml
Nutrients and their daily requirements • Electrolytes and vitamins are added to the daily requirements • These basal requirements are increased in catabolic states (disease, trauma and pyrexia), e.g. 15-50% increase following peritonitis.
Aetiology of malnutrition INADEQUATE INTAKE OF NUTRIENTS • Anorexia: cancer, severe sepsis, liver disease, etc • Dysphagia: lesions of the tongue, pharynx, oesophagus, stomach. • Prolonged coma
Causes of malnutrition (cont’d) IMPAIRED ABSORPTION OF NUTRIENTS DUE TO INTESTINAL MALFUNCTION • Persistent vomiting: e.g. gastric outlet obstruction, paralytic ileus, peritonitis, intestinal obstruction. • Poor absorption: Massive bowel resection, Chrohn’s disease, Ulcerative colitis.
Causes of malnutrition (cont’d) EXCESSIVE LOSS OF NUTRIENTS • Persistent vomiting • Diarrhoea • Enterocutaneous fistulae
Aetiology of malnutrition (cont’d) EXCESSIVE CATABOLISM • Due to metabolic changes caused by inflammatory mediators in trauma, burns and sepsis
Pathophysiology of malnutrition Normal feeding-fasting cycle • Secretion of insulin: -Postprandial deposition of glycogen and fat -Protein synthesis • In fasting, ↓ insulin ↑glucagon: -Mobilization of glucose from glycogen -Lipolysis -Proteolysis
Pathophysiology of malnutrition Starvation • The “obligate glucose users” (brain, nerve cells, Rbc, PCT cells) require 160g of glucose/day . • Body’s glycogen can last only 12hrs • Therefore gluconeogenesis from metab of lactate(Cori cycle), glycerol(Lipolysis) and AAs(Proteolysis) in The liver and Kidney is necessary • During prolonged starvation, brain adapts to use of Ketone bodies for energy
Pathophysiology of malnutrition • In the previously fit subject complete starvation causes death in 60-70days after loss of 30-40% of the initial body weight due to irreversible organ impairement
Pathophysiologycon,td • Calculating deficits. • Determining daily requirements. • Ongoing losses. Energy Requirements. Basal EE: (using Harris-Benedict equation). Male=[66.5+(13.7×wt kg)+(5×ht cm)- (6.7×age yr)]×AF×IF Female=[66.51+(9.6×wt kg)+(1.8×ht cm)- (4.7×age yr)]×AF×IF
Calculating deficits. Determining daily requirements. Ongoing losses. Energy Requirements. Basal EE: (using Harris-Benedict equation). Male=[66.5+(13.7×wt kg)+(5×ht cm)- (6.7×age yr)]×AF×IF Female=[665.1+(9.6×wt kg)+(1.8×ht cm)- (4.7×age yr)]×AF×IF Stress factor/Illness factor: additional energy expenditure caused by pts illness. Low stress = 1.2 Moderate stress = 1.2-1.3 Severe stress = 1.3-1.5 Burns = 2.0
Total Energy Expenditure=BEE × stress factor × activity factor • Energy Exp. of Activity • 1.3x BEE ambulatory. • 1.2xBEE bedridden. • 1.1 x BEE ventilator.
ASSESSMENT OF NUTRITIONAL STATUS Lucid history: • Nutritional history • Recent illness (diarrhoea, vomiting) • Recent weight loss (>10% B. wt) • Weakness, • inability to perform normal functions
ASSESSMENT OF NUTRITIONAL STATUS (cont’d) Thorough examination: • Pallor, • oedema, • Anthropometry:- B. wt <80% of ideal wt for height BMI: Wt (kg)/(Ht meters)2 Normal= 19-25kg/m2 Mid arm muscle circumf: < 80% of expected value Triceps skin fold thickness (callipers) BIA (Bioelectric impedance analysis) • Measurement of function Hand grip dynamometer (using the non-dominant hand) Respiratory function tests
ASSESSMENT OF NUTRITIONAL STATUS (cont’d) Laboratory tests • Serum albumin <30g/L • Total lymphocyte count <1.2 x 109/L • Others: Serum transferrin, thyroxin-binding prealbumin, folic acid, B12, 25-hydroxy vitamin D, etc.
aims of Nutritional Support provide adequate nutrition in disease or after surgical trauma by providing:- • Adequate energy for the body’s metab needs • AAs for protein synthesis • Substrates for gluconeogenesis to support the “obligate glucose users”(brain, nerves, Rbcs, PCT cells, inflam cells) • Daily Rqts of H2O & electrolytes.
ROUTES FOR FEEDING • There are two principal routes:- • Enteral Stomach, jejunum • Parenteral Peripheral vein, Central vein The enteral route in preferred:
Enteral Feeding • This is the preferred route: It is cheap, more physiologic, prevents translocation by promoting gut mucosal defense
Enteral Feeding Enteral feeding is by: • Mouth (natural route) • Tube feeding: Nasogastric tube Naso-enteral tube – Vygon, Roussel, Clinifeed tubes • Ostomies Open (feeding) gastrostomy: Stamm/ Witziel tech Open (feeding) jejunostomy: Stamm/ Witziel tech Percutaneous endoscopic gastrostomy (PEG) Percutaneous endoscopic jejunostomy (PEJ)
Enteral Feeding Examples of enteral feeds • Blenderized diet • Elemental diet • Special purpose formulation (disease specific) diet Formulations: Liquids- Isocal, clinifeed, favour, nutrauxil Powders- Flexical, casilan, complan, etc
Enteral Feeding Complications • Tube related blockage, fracture, displacement, bowel perforation, Reflux leading to aspiration pneumonitis • Feed related Severe diarrhoea with fluid/elect imbalance Hyperglyceamia
Parenteral Nutrition • Parenteral nutrition is necessary when there is intestinal failure (the gut is unable to digest and absorb adequate amount of nutrients to meet the body’s needs). • The nutrients are delivered i/v • Isotonic solutions: Via Peripheral vein • Hypertonic solutions: Via Central vein
Parenteral Nutrition Examples of parenteral solutions • CHO solutions glucose, sorbitol, xylitol, fructose • Fat solutions 10% and 20% emulsions of soya oil • Amino acid solutions Crystalline (synthetic) amino acids
Parenteral Nutrition • Admin is via fine polyurethrane catheters threaded into a peripheral or central vein and delivered based on a strict infusion protocol under aseptic technique
Parenteral Nutrition Observations of patient • Daily clinical exam • Fluid input/output • Daily weighing • U/E/PH, clotting studies every 48hrs • Twice weekly blood glucose • Weekly LFTs, FBC, and Calcium
Parenteral Nutrition COMPLICATIONS • Acute reactions to fat and AA solutions • Thrombophlebitis • Osmotic diuresis • Reduction in myocardial contractile force if infused rapidly • Septicaemia • Metabolic acidosis • Hypophosphataemia • CCF • Catheter malposition • Hyperglycaemia etc
Hyperalimentation Parenteral hyperalimentation: • The intravenous delivery of nutrients to the malnourished patient in a state of hypercatabolism in amounts as high as two and a half times the basal (resting) requirements of a healthy individual of the same body size and surface area so as to achieve a level of nutrition 40%-50% above the nitrogen equilibrium so as to convert the patient into anabolic state.
CONCLUSION • The success or otherwise of nutritional support should be determined by tolerance to nutrients • It is unrealistic to expect nutritional support to alter the natural history of disease • It is imperative that nutrition related morbidity is kept to a minimum • Nutritional support are fundamental to good surgical practice