Download
1 / 23
230 likes | 305 Vues
Explore the impact of financial incentives on organ donation, facing challenges and objections while aiming to increase donor response for a critical cause.

E N D
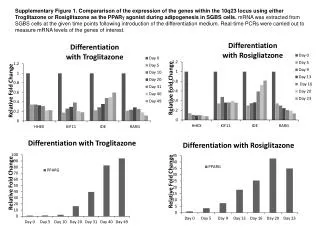
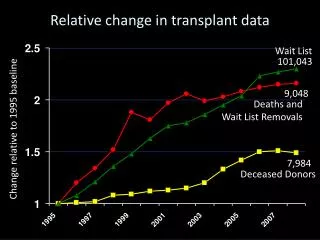
Relative change in transplant data Wait List 101,043 9,048 Deaths and Wait List Removals Change relative to 1995 baseline 7,984 Deceased Donors
What To Do? • All efforts so far: nibbling at the edges • Dramatic, effective change is needed • If there are insufficient volunteers to work • construction atop skyscraper • as diplomat in dangerous 3rd world country • other undesirable jobs • How do we volunteers? • We pay them more
Financial Incentives (FI) • We should • make all reasonable efforts to organ donation • “reasonable” defined by evidence, not by emotions • study FI for deceased donations w pilot studies • FI not intrinsically unethical (benefits:harms) • pilot studies can measure benefits:harms • pilot studies in limited area (1 state or small group) • Change NOTA, based on high benefits/harms • FI highly effective in every sector of economy b/c they expand options in personal lives
Reasons Not to Donate • Desire to bury body intact (religion, own belief) • Avoidance of confronting loss, own mortality • Distrust of medical community • Belief that allocation is not equitable • Misunderstanding of tx effectiveness • Lack of understanding of brain death • Stresses at time of sudden unexpected death
NOTA Allows 1 Reason to Donate The sole permissible incentive: Service to others (altruism)
Objections to FI for Deceased Donors Main objections: • FI Will Harm/Benefit, Organ Donation • FI will undermine social fabric • dilute desirable spirit of altruism • commodify human body parts • introduce coercion, voluntariness
FI Will Harm/Benefit: Organ Donation • Donation b/c $$$ anger/insult • BUT, ppl familiar w payment for valuable goods • We can measure this in pilot study
FI Will Undermine Social Fabric:Dilute Desirable Spirit of Altruism • Impulse to do good not binary (all-or-none) • most ppl part altruist, part self-interested • FI might add enough motivation to persuade • Motivation variable, law blunt instrument • FI: token of societal gratitude (=tax incentives) • Level of social cohesion measurable!
FI Will Undermine Social Fabric:Commodify Human Body Parts • Donors of blood and other tissues paid • no compelling ethical distinction from organs • Donation implies property rights in organs • “One cannot give away what one does not own any more than one can sell it” (AMA 1995) • Recipients pay for organs—only the donor does not benefit financially! • Type of FI & $ amt regulated, no organ bazaar
FI Will Undermine Social Fabric:Coercion Voluntariness • Informed consent must be voluntary • FI more likely poor to donate, so • burden of donation on poor un =, unfair • Circumstances of poor make FI coercive • BUT, well-off don’t clean toilets, pick berries • we don’t ban toilets and berries • we allow free choice, make conditions safe • What is coercion? In context of free society: • Forcing others to do what they would not otherwise do. So FI not coercive.
Inferences • FI not intrinsically unethical • FI acceptable when benefits/harms positive • every fear about FI based on assumptions • yet, effects of fears about FI measurable • no good reason to prohibit pilot study of FI • policy/law then based on evidence, not emotion • Pilot studies must be ethically designed • sound science, measurable outcomes, set time • FI moderate value, lowest level to donation • FI only for deceased donors, not living • no buying organs: allocation by UNOS algorithms
FI for Pilot Studyfor SC or Region 11 • Examples, (likely) most to least effective: • Deposit of $1,000-5,000 into donor’s estate • Estate tax credit $10,000 • Funeral expenses up to $5,000
The case for FI fundamentally a moral one: • Which is morally preferable: • prohibit FI because society might degenerate or more poor might choose to donate • offer $1,000-5,000 and save up to 8 lives for every new donor
Relative change in transplant data A Final Word Wait List 101,043 “We have never encountered a single policy more at odds with public welfare than the current [altruism-only] organ procurement policy in the United States . . . If the current policy is maintained, the shortage will continue to grow worse, as will the needless suffering. 9,048 Deaths and Wait List Removals Change relative to 1995 baseline 7,984 Deceased Donors --Blair and Kaserman, Yale Journal of Regulation, 1991
Rapid Organ Recovery Ambulances Update Last Updated: Thu, 11/19/2009 - 1:57pm Early in 2008, Judicial Watch initiated an investigation of a government sponsored organ procurement program. The program, known as Rapid Organ Recovery Ambulances (RORA), was administered in New York City and received funding from the Health Resources and Services Administration of the Department of Health and Human Services. As highlighted in a June blog series, the program breached ethical and medical standards, discriminately targeted minorities, and raised institutional credibility questions. As part of its investigation, Judicial Watch sued the Fire Department of New York (FDNY) and reached a favorable settlement after FDNY obfuscated transparency by not disclosing related records. Following its publications on this dubious program, Judicial Watch continued to follow-up to receive the actual program data. Judicial Watch recently received some additional documents that further shed light on the program and demonstrate the power of public exposure. Many of the program goals for which RORA was funded have yet to be met. As noted in a previous blog entry, the ethical White Paper that was slated to be written by February 2008 has yet to be written as of October 2009. According to HRSA's letter, data from the ambulance and procurement activities have yet to be gathered as “there have been no ambulance or EMS dispatches for rapid organ recovery.” On one hand, readers should be relieved that the program has yet to actually be put into action. On the other hand, however, the US government provided millions of dollars based on a proposal that was not fully carried out. The documents provided do not demonstrate that HRSA stopped funding RORA even after the White Paper was not provided. The documents further do not demonstrate where the money actually went … http://www.judicialwatch.org/foiablog/2009/nov/rapid-organ-recovery-ambulances-update.
Donation-procurement steps • Take referral call • Assess potential donor • Talk with family, request donation • Manage donor in ICU • Place organs (UNOS algorithm) • Move donor to OR, manage surg teams • Package, ship organs • Complete all paperwork
Basic strategy: division of labor, specialized personnel • Family Support Counselor (counseling, nursing) • emotional support • education (brain death, value of tx) • Nurse Clinician (ICU nurse) • manage donor in ICU • Organ Recovery Coordinator (OR nurse/tech) • manage donor in OR, distribute organs • Clinical Services Liaison (business PR/sales) • staff education • record review • Aftercare Counselor (counseling) • follow-up counseling, support groups, satisfaction surveys
HRSA Transplant Center Growthand Management Collaborative • Best Practices Evaluation (2003-2007) • Institutional Vision And Commitment • Dedicated Team • Aggressive Clinical Style • Patient And Family Centered Care • Aggressive Management of Performance Outcomes
Donation Rate by Year 60 50 40 Donors per million of population 30 20 10 All OPO's 2 S.D. Lifepoint 0 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 Year
Origin of Prohibition of FI • UAGA 1968: no ban on selling/buying • Cyclosporine tested 1979, clin use 1982 • Tx rapidly → growth industry • Organ entrepreneurs • NOTA 1984: no “valuable consideration” • harms of pmnt substantially outweigh benefits • Benefits:harms has changed in last 20 yrs
Sources of Organs for Tx • Deceased donors (brain death) • Living donors • Donors after cardiac death • Xenografts • De novo organs (regenerative technologies) Greatest potential gain with least ethical controversy