Download
1 / 1
10 likes | 148 Vues
Changes in Opioid Use Over One Year in Patients with Chronic Low Back Pain. Alejandra Garza, Gerald Kizerian, PhD, Sandra Burge, PhD The University of Texas Health Science Center at San Antonio. Introduction. Results.

E N D
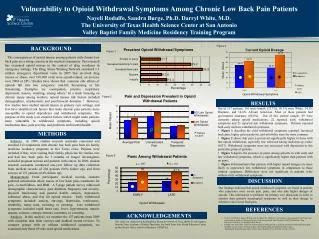
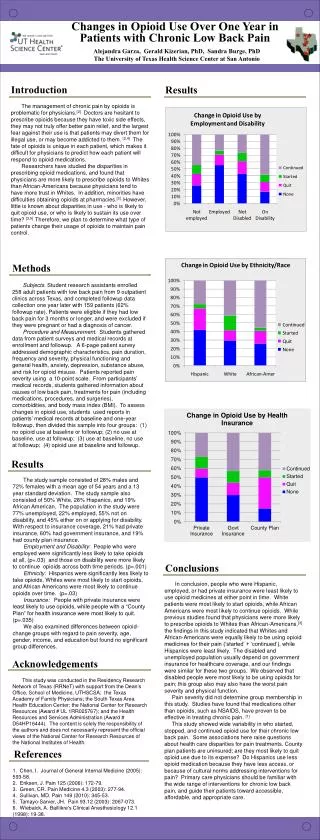
Changes in Opioid Use Over One Year in Patients with Chronic Low Back Pain Alejandra Garza, Gerald Kizerian, PhD, Sandra Burge, PhD The University of Texas Health Science Center at San Antonio Introduction Results The management of chronic pain by opioids is problematic for physicians.[2] Doctors are hesitant to prescribe opioids because they have toxic side effects, they may not truly offer better pain relief, and the largest fear against their use is that patients may divert them for illegal use, or may become addicted to them. [2,4] The fate of opioids is unique in each patient, which makes it difficult for physicians to predict how each patient will respond to opioid medications. Researchers have studied the disparities in prescribing opioid medications, and found that physicians are more likely to prescribe opioids to Whites than African-Americans because physicians tend to have more trust in Whites. In addition, minorities have difficulties obtaining opioids at pharmacies.[3].However, little is known about disparities in use - who is likely to quit opioid use, or who is likely to sustain its use over time? [3,5] Therefore, we plan to determine what type of patients change their usage of opioids to maintain pain control. Methods Subjects. Student research assistants enrolled 258 adult patients with low back pain from 9 outpatient clinics across Texas, and completed followup data collection one year later with 159 patients (62% followup rate). Patients were eligible if they had low back pain for 3 months or longer, and were excluded if they were pregnant or had a diagnosis of cancer. Procedure and Measurement. Students gathered data from patient surveys and medical records at enrollment and followup. A 6-page patient survey addressed demographic characteristics, pain duration, frequency and severity, physical functioning and general health, anxiety, depression, substance abuse, and risk for opioid misuse. Patients reported pain severity using a 10-point scale. From participants’ medical records, students gathered information about causes of low back pain, treatments for pain (including medications, procedures, and surgeries), comorbidities, and body mass index (BMI). To assess changes in opioid use, students used reports in patients’ medical records at baseline and one-year followup, then divided this sample into four groups: (1) no opioid use at baseline or followup; (2) no use at baseline, use at followup; (3) use at baseline, no use at followup; (4) opioid use at baseline and followup. Results The study sample consisted of 28% males and 72% females with a mean age of 54 years and a 13 year standard deviation. The study sample also consisted of 50% White, 28% Hispanics, and 19% African American. The population in the study were 77% unemployed, 22% employed, 55% not on disability, and 45% either on or applying for disability. With respect to insurance coverage, 21% had private insurance, 60% had government insurance, and 19% had county plan insurance. Employment and Disability: People who were employed were significantly less likely to take opioids at all, (p=.03) and those on disability were more likely to continue opioids across both time periods. (p=.001) Ethnicity: Hispanics were significantly less likely to take opioids, Whites were most likely to start opioids, and African Americans were most likely to continue opioids over time. (p=.03) Insurance: People with private insurance were least likely to use opioids, while people with a “County Plan” for health insurance were most likely to quit. (p=.035) We also examined differences between opioid-change groups with regard to pain severity, age, gender, income, and education but found no significant group differences. Conclusions In conclusion, people who were Hispanic, employed, or had private insurance were least likely to use opioid medicines at either point in time. White patients were most likely to start opioids, while African Americans were most likely to continue opioids. While previous studies found that physicians were more likely to prescribe opioids to Whites than African-Americans,[3]. the findings in this study indicated that Whites and African-Americans were equally likely to be using opioid medicines for their pain (‘started’ + ‘continued’), while Hispanics were least likely. The disabled and unemployed population usually depend on government insurance for healthcare coverage, and our findings were similar for these two groups. We observed that disabled people were most likely to be using opioids for pain; this group also may also have the worst pain severity and physical function. Pain severity did not determine group membership in this study. Studies have found that medications other than opioids, such as NSAIDS, have proven to be effective in treating chronic pain. [1] This study showed wide variability in who started, stopped, and continued opioid use for their chronic low back pain. Some associations here raise questions about health care disparities for pain treatments. County plan patients are uninsured; are they most likely to quit opioid use due to its expense? Do Hispanics use less opioid medication because they have less access, or because of cultural norms addressing interventions for pain? Primary care physicians should be familiar with the wide range of interventions for chronic low back pain, and guide their patients toward accessible, affordable, and appropriate care. Acknowledgements This study was conducted in the Residency Research Network of Texas (RRNeT) with support from the Dean’s Office, School of Medicine, UTHSCSA; the Texas Academy of Family Physicians; the South Texas Area Health Education Center; the National Center for Research Resources (Award # UL 1RR025767); and the Health Resources and Services Administration (Award # D54HP16444). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources of the National Institutes of Health. References 1. Chen, I. Journal of General Internal Medicine (2005): 593-58. 2. Eriksen, J. Pain 125 (2006): 172-79. 3. Green, CR. Pain Medicine 4.3 (2003): 277-94. 4. Sullivan, MD. Pain 149 (2010): 345-53. 5. Tamayo-Sarver, JH. Pain 93.12 (2003): 2067-073. 6. Wiebalck, A. Baillikre's Clinical Anesthesiology 12.1 (1998): 19-38.