Download
1 / 29
290 likes | 305 Vues
Explore the significance of UKCRN, MCRN, and CCRN in supporting paediatric research, with insights into network structures, funding, staff roles, and study portfolios. Learn how these networks streamline research management and provide essential NHS infrastructure. Discover the diverse therapeutic areas covered and the impact on clinical trials in paediatrics.

E N D
NIHR Clinical Research Networks – what they mean for paediatrics Rosalind L Smyth, Director MCRN
Plan of talk • UKCRN and the history. • MCRN – brief update. • Comprehensive Clinical Research Network. • Implications for organisation and support of paediatric research.
UK Clinical Research Network Comprehensive Research Networks
National Cancer Research Network • Established 2001 • Coordinating Centre in Leeds • 40 Local Research Networks across the UK • Total population 60.2 million (100% coverage) • 474 studies in the portfolio
National Cancer Research Network Comparison of recruitment into Myeloma VII (pre-NCRN) and Myeloma IX (post-NCRN)
National Cancer Research Network Accrual to NCRN Portfolio studies Across the UK
Introduction of Clinical Research Networks FIRST PHASE NCRN 2000~£20M MHRN2003~£ 4M SECOND PHASE (TCRN’s) MCRN, DRN, SRN, DeENDroN 2005~£16M THIRD PHASE Primary Care Research Network 2007~£ 2MComprehensive Research Network 2007~£90M+
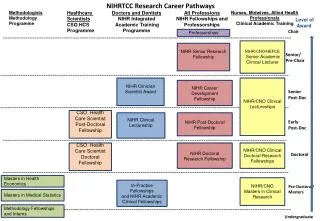
Rosalind Smyth Director Information Systems Chris Braithwaite Clinical Trials Unit Four core staff Paula Williamson Portfolio Manager To be appointed Industry Liaison Officer Andrew Rose Tony Nunn Training & Education Sarah McCauley David Edwards Assistant Director Vanessa Poustie Consumer Involvement Jenny Preston Nicola Madge/NCB Clinical Studies Groups Jennifer Blakeburn Administrative support Moira Saphier Kathy McKenna Neonatal Network Coordinator Sara Lewis NPEU MCRN Co-ordinating Centre – Organogram and Workstreams
MCRN Local Research Networks Cheshire, Merseyside & North Wales Greater Manchester, Lancashire & S.Cumbria West Midlands Trent South West SENCE
MCRN Local Research NetworksFunding: each LRN, £500K per annum LRN Director UKCRN MCRN Local Clinical Leads LRN Manager Infrastructure support funding also includes service support costs in the NHS Research staff 1 Administrator 6-7 Research Officers Pharmacist Other support staff Formulations Scientist (in 3 LRNs)
MCRN Clinical Studies Groups Allergy,Nephrology, Infection & ImmunityDr Mike Sharland Anaesthesia, Pain, Intensive Care, Cardiology (APICC) Dr Robert Tasker Diabetes, Endocrinology & Metabolic MedicineProf David Dunger Gastroenterology, Hepatology & NutritionDr Stephen Murphy General Paediatrics (including Dermatology)Dr Colin Powell Methodology Prof Peter Brocklehurst NeonatalProf David Field Neurosciences Dr William Whitehouse Pharmacy & PharmacologyProf Ian Wong Respiratory & Cystic FibrosisProf Jonathan Grigg Rheumatology (MCRN/arc) Dr Michael Beresford Children’s Cancer and Leukaemia Group (CCLG)Dr Bruce Morland
What is the UKCRN Portfolio? • A national register of all eligible studies • DH have defined ‘eligible’ for England – NIHR portfolio • Emphasis on national competitive funding and external peer review • Portfolios in Northern Ireland, Scotland and Wales • Aim is UK-wide working within portfolios • multi-centre and single centre • commercial and non-commercial Details of current portfolio available on UKCRN website (www.ukcrn.org.uk) (in development)
MCRN Portfolio Studies • 51 studies adopted into Network • 40 Non-commercial • 11 Commercial - 9 different companies • Studies at different stages • Many different therapeutic areas • UKCRN Portfolio Database • More studies in pipeline
Comprehensive Clinical Research Network (CCRN) • to provide the NHS infrastructure to support clinical research-25 CLRNs • streamline the research management function--reduce bureaucracy where possible • Inclusive of all healthcare • From April 2009 will be the main route for NHS service support for clinical research
What is a Comprehensive Local Research Network? • Primary vehicle for NHS infrastructure (service support) • Primary, secondary and tertiary care and MH • Clinical Director and Network Manager and core team • Network Executive and Network Board • Host organisation • Research management for portfolio • A typical CLRN: - NHS staff – management, sessions forclinicians, nurses, data managers, secretarial. - infrastructure in primary care. - diagnostics and service costs. - running costs.
CLRN- A balance between national standards and consistency and local ownership and control! Geography-functional clinical research entities Host Organisations Clinical Directors Network Boards Network manager/Core Teams NHS Infrastructure (money) Done quickly and in parallel—for patients and staff (April –October 2007)
Resources • Stage 1- Allocated to all networks asap • Core team (5 posts) ~ 300k pa per CLRN) £200k (07/08) • Per capita allocation (~1.5M per 2M pop) £750k (07/08) • Research management and governance • Research Infrastructure (includes sessions for clinicians) • Does NOT include non-staff clinical support costs (eg radiology, pharmacy and pathology) • 2006/7 pro-rata allocation based on roll-out • In addition to existing transition funding and TCRN funding • Stage 2 – from April 2008 • Activity based • Increased operational staff • Non-staff support costs • Rising to £90M pa … any necessary increases thereafter
PROPOSALS FOR SUPPORTING TOPICS WITHIN CCRN NHS INFRASTRUCTURE an example for Respiratory Health STUDIES Lead Functions Local INDUSTRY LINKS; ADOPTION; ADVICE; FEASIBILITY. National
Figure 2 STUDIES NHS INFRASTRUCTURE Local National PORTFOLIO GENERATION IN ACADEMIC SECTOR Portfolio Development FUNDERS PROVIDE PRIORITIES AND SUPPORT Short Term Groups
How will non-medicines paediatric research (NMPR) be represented within CCRN? • Currently NMPR is not recognised within UKCRC/UKCRN topic lists. • Concerns about this have been expressed locally and nationally. • UKCRN have asked MCRNCC if they wish to become involved in the co-ordination of NMPR studies across England. • This has been discussed at the MRCN Executive and Board who were unanimous in support of this proposal. • MCRN will ensure that their core business continues to get high priority, but can use the infrastructure and links developed to support all paediatric research.
Proposal to Co-ordinate NMPR • Currently under discussion between MCRN, UKCRN and DH. • Actively being discussed at local level, and with national organisations: RCPCH, Children’s Research Alliance, APA, BAPs etc. • CLRN Directors will be involved in identifying level of interest and strengths in their CLRN. • Full discussion planned at a meeting in 2008, to include CLRN representatives and all stakeholders.
Conclusions • Pace of change is very rapid. • Huge opportunities – need to be recognised and grasped. • Broad support but an anxious research management community. • Could become the best whole system for clinical research in the world. • For paediatrics, we must build on achievements and position ourselves well for the future. • All help and advice gratefully received