MALE INFERTILITY
1.25k likes | 3.69k Vues
MALE INFERTILITY. AMIT K SHARMA UROLOGIST HSB. At the end of this talk 1.Understand the performance characteristics of Semen Analysis 2.Describe the role of semen analysis in prognosticating pregnancy, and consequently its utility in defining fertility .

MALE INFERTILITY
E N D
Presentation Transcript
MALE INFERTILITY AMIT K SHARMA UROLOGIST HSB
At the end of this talk • 1.Understand the performance characteristics of Semen Analysis • 2.Describe the role of semen analysis in prognosticating pregnancy, and consequently its utility in defining fertility
3.Understand the role of semen analysis as a marker for significant underlying disease • 4.Provide evidence-based recommendations to your patients
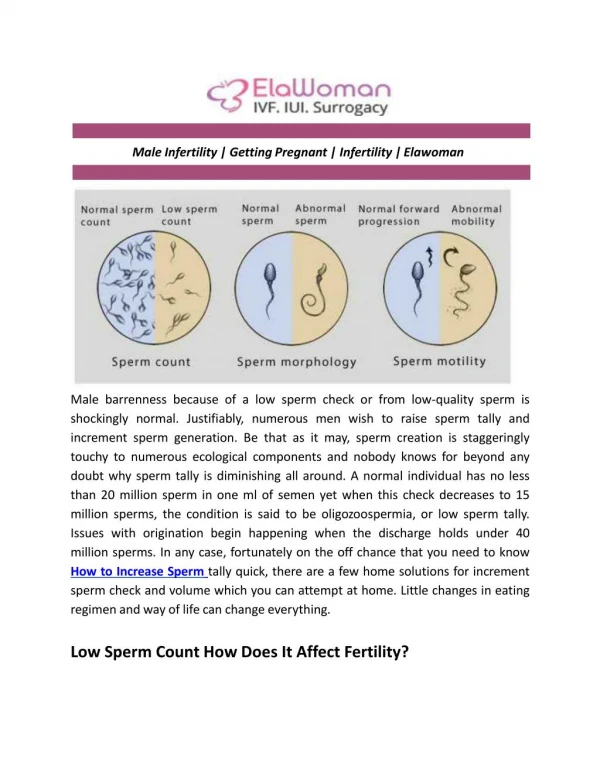
Semen Analysis - Introduction • Primary infertility affects approximately 15% of couples with male factor infertility accounting for 50% of cases • Semen analysis has traditionally been the initial test of choice in the evaluation of the infertile male.
What is Semen? Sperm + Seminal Plasma Source Volume 1.Testis/vas <0.1 ml 2.Epididymis 3.SV 1.5-2.0 ml 4.Ampullae 5.Prostate 0.5 ml 6.Bulbourethral glands 0.1 ml 7.Glands of Littre 0.1 ml
Because the human spermatozoa show marked heterogeneity, at least two semen samples should be evaluated • collected at least 7 days between specimens • 3 months after any febrile illness. • Samples are collected after a period of abstinence of greater than 48 h • Specimens should be analyzed within 1 h of collection • as semen liquefies at room temperature within 60 min
If the results of semen analysis are normal according to WHO criteria, one test should be sufficient • If the results are abnormal in at least two tests, further andrological investigation is indicated
Natural conception may occur for men even when SA values are less than WHO reference ranges and, conversely, men with normal SA parameters may have difficulty initiating a pregnancy.
Biological Variation • A 33 yo male with a 1 year history of infertility presents to your clinic today and provides a SA. History and physical are unremarkable. Partner is normal • On questioning, he abstained for 1 day before providing a semen analysis
Volume 2.5 cc • Concentration 15 million/ml • Motility 60% • Morphology 8%
Questions • 1.Does the season matter? • 2.Would have abstaining for longer time have made a difference? If so, how much of a difference? • 3.Does it matter how many times he ejaculated last week
4.If he repeated the SA the exact same way several times, how much variation would there be? Would some of the parameters vary more than the others? • 5.He’s 33 now. Would his results have been different last year
1. Does the season of collection matter? A: MAYBE (sperm maybe best in spring) • 2. Would have abstaining for longer time have made a difference? A: DEFINITELY (by about 25% per day up to day 4) • 3. Does it matter how many times he had intercourse last week? A: MAYBE (less than 1-2/7 days may maximize)
4. How much difference between could you expect with between 2 samples. • A: A LOT (about 30-50% CV in all parameters between 2 samples) • 5. Would his SA likely have been any different when he was younger? • A: NO (except for the volume)
Definations • Infertility is a disease defined by the failure to achieve pregnancy after 12 months or more of regular unprotected intercourse • Fertility is defined by the actual production of live children • Sterility is the absence of the capacity to reproduce
Conception rates • Per cycle is 25% • Per year 85% • Therefore, 10-15% of couples meet the definition of infertility
INFERTILITY ≠ ABSENCE OF FERTILITY INFERTILITY ≠STERILITY INFERTILE OFTEN BECOME FERTILE
Prognostic Performance of SA for Pregnancy Starting at TIME 1 YEAR (i.e. Infertile) • Approximately 29%of couples with concentrations of <20 x106/ml will conceive within 2 years of being declared ‘infertile’ (Collins Fertil Steril 1995)
Approximately 27% of couples with total motile counts <5 x106/ml will conceive within 2 years of being declared ‘infertile’ (Snick Human Reprod 1997) • If the SA is within the reference range, the probability of conception is 50-70% within 2-3 years
Drawbacks • There are still a significant proportion of patients with normal semen analyses but with unexplained infertility. • A normal spermiogram does not necessarily correlate with fertility potential, because it does not assess sperm function. • Standard semen analysis has been unable to detect some functional deficiency in about 40% of men presenting for sub-fertility
Semen analysis is not a diagnostic test for infertility or fertility • Semen analysis parameters are crude prognosticators of fertility. Concentration and morphology are the strongest parameters.
Don’t rely on the ‘reference range’ on the SA report • Even using everything which is currently measurable, only a small portion of the probability of future success can be prognosticated.
Male Infertility Causes • Idiopathic male infertility 31 % • Maldescendedtestes 7.8 % • Urogenital infection 8.0 % • Disturbances of semen deposition and sexual factors 5.9 %
General and systemic disease 3.1 % • Varicocele 15.6 % • Hypogonadism 8.9 % • Immunological factors 4.5 % • Obstructions 1.7 % • Other abnormalities 5.5%
Classification • I.Non obstructive infertility 60%: inadequate sperm production by the testes • II. Obstructive infertility 38%: normal sperm production but there is a blockage in the genital tract • III. Coital infertility 2%: normal sperm production and patent genital tract; however infertility is secondary to sexual dysfunction which impairs intromission or ejaculation.
Causes Of Non Obstructive Infertility • Hormonal -HypogonadotrophicHypogonadism -Thyroid gland disorders -Hyperprolactinaemia • Genetic - Y Chromosomal microdeletions,translocations and aneuploidy - KS
Varicocele • Undescended testis • Gonadotoxins • Systemic illness • Orchitis,torsion,trauma and tumours • Autoimmune infertility
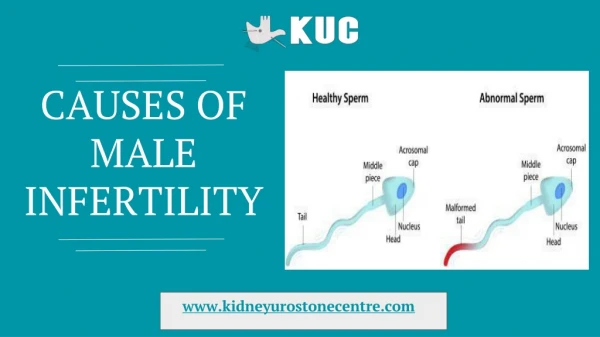
Severe Male Factor Infertility • number < 1 m/ejaculate • motility < 20% • progression < 2/4 • abnormal forms > 85%
Structural and chromosomal abnormalities found in 5 % infertile man and 14% azospermic man • In addition to the SRY gene which is involved in determining the fate of the embryonic bipotential gonad, the Y chromosome also contains the ‘‘male-specific Y’’ (MSY) which contains chromosomal material not represented elsewhere in the genome and contains numerous genes involved in spermatogenesis
An AZFc microdeletion quantitatively impairs spermatogenesis however men with such deletion may be oligozospermic and even father children naturally • Unlike AZFc microdeletion; AZFa and AZFb microdeletions are associated with azoospermia and complete spermatogenic failure and sperm will not be found in the testes of men with these deletions via surgical sperm retrieval (TESE)
Klinefelter syndrome (KS) is the most common example of a numerical abnormality • KS is associated with primary testicular failure, patients present with hypogonadal features, azoospermia, gynecomastia,small sized testes and some may have learning difficulties.
Micro-TESE yields sperm in up to 50% of cases with a 30—50% pregnancy rate via ICSI • The younger the age of male the better the TESE outcome, so it has been suggested that TESE should be performed on KS patients before the age of 35 years
How do Y deletions cause maleinfertility Code for proteins essential for spermatogensis
Causes of Obstructive Infertility • Intratesticular obstruction • Epididymal Obstruction • CBAVD • EDO • Vasectomy-post hernia surgery, orchidopexy
Coital Infertility • ED • PE • Penile deformities • Anejaculation • Retrograde Ejaculation
History • Time the couple has been engaging in unprotected intercourse and how long they have been deliberately trying to conceive • The frequency and timing of vaginal intercourse with respect to the female partner’s menstrual cycle should be assessed • Technically, the infertility diagnosis only applies to couples engaging in unprotected vaginal intercourse at least twice a week on average for a year, although evaluation may occur earlier when the female partner is older than 35 years
Primary or secondary infertility • Medical Conditions • Lifestyle factors • Medications • Infection and inflammation • Surgery
Family History • Female factors female partner age(age greater than 35 years suggests greater likelihood of fertility impairment), menstrual cycle regularity, increased serum anti-mu¨llerian hormone or day 3 serum FSH and pregnancy history
Physical Examination -Secondary sexual characteristics -Penis -Testis -Epidydimis -Cord
Investigations • SFA • Hormonal Profile • Ultrasound Scrotum & Testis • TRUS