Download
1 / 21
260 likes | 1.36k Vues
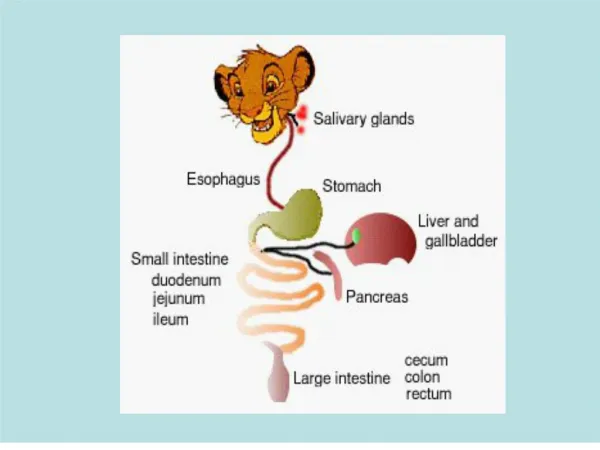
Gastro-Intestinal Tubes & Enteral Nutrition . NURS 108 Majuvy L.Sulse MSN, CCRN. Enteral Feeding. Nutrients given via the GI tract Easier to give especially for home care Types: Polymeric-1 to 2kcal/ml-milk based blenderized foods prepared by the dietary or at home

E N D
Gastro-Intestinal Tubes & Enteral Nutrition NURS 108 Majuvy L.Sulse MSN, CCRN
Enteral Feeding • Nutrients given via the GI tract • Easier to give especially for home care • Types: • Polymeric-1 to 2kcal/ml-milk based blenderized foods prepared by the dietary or at home • Modular-3.8 to 4kcal/ml-single and incomplete formulas • Elemental-1 to 3kcla/ml predigested nutrient formulas for a partially functional GI to absorb • Specialty formulas-1 to 2 kcal/ml-formulas designed to meet specific needs in certain illness.
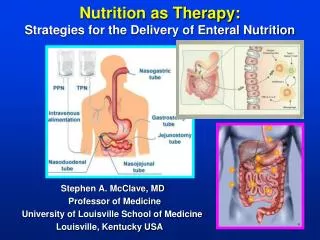
Feeding Tubes • Nasoenteric tubes (NET)- usually for short term <4 weeks • Nasogastric (NGT)- • Nasointestinal-doudenal or jejunal (NDT/NJT) • Surgically placed (enterostomal) gastrostomy & Jejunostomy tubes-long term use • Endoscopic • gastrostomy (PEG) • Jejunostomy (PEJ)-bypass stomach in presence of gastric disease, UGI obstruction, abnormal gastric or doudenal emptying
Feeding Tubes • Nasointestinal tubes are longer than NG tubes and are indicated to medically treat an obstruction of the small intestine in someone who's a very poor surgical risk. They rely on a weighted distal end and peristalsis to advance the tube along the intestinal tract in an attempt to relieve the obstruction
Indications for Enteral feedings • Inadequate oral intake • Continuous feedings • CVA • Difficulty swallowing-absence of gag reflex • Anorexia Nervosa • Severe depression • Local trauma or critical illness • Prolonged intubation • Gastrointestinal disorders • Fistulas, IBD, mild pancreatitis
Indications for Enteral feedings • Neurological and mascular disorders • Brain neoplasm • CVA • Dementia • Myopathy • Parkinson’s disease • Cancer • Upper GI • Head & Neck
Nursing Management • Patient position • HOB 30-45 degrees • Patency of tube • Irrigate with water before and after each feeding (if intermittent) or medication administration • Tube position • Check tube placement before each feeding and drug administration • Xray –most accurate assessment of placement • Aspirate gastric contents • Check pH contents-less than 5 indicative of stomach contents • Check every 4-8 hours with continuous feedings • Check for bowel sounds
Nursing Management • Formula • Given at room temperature • Amount in bag should not exceed 4 hours or per policy • Labeled with date and time initially used • Aspirate contents & measure amount-if volume is >200 ml with signs of intolerance, hold feeding for an hour and recheck residual volume. Aspirate should be re-instilled.
Nursing Management • Feeding administration-rate & volume increased gradually to minimize side effect as nausea & diarrhea. Water flushes or boluses given • Feeding pump-continuous • Gravity method-intermittent-volume is usually 200-500/feeding • Nursing care • Daily weights or as per policy • I/O • Blood glucose • Oral care
Complications related to Tube Feedings • Vomiting or aspiration • Improper tube placement • Delayed gastric emptying • Contamination of formula • Diarrhea • Feeding too fast, hypertonic formula, medications • Lactose intolerance • Contamination of formula • Low fiber formula
Complications related to Tube Feedings • Constipation • Formula components • Poor fluid intake • Drugs • Impaction • Dehydration • Excessive diarrhea • Poor fluid intake • Hyperosmotic diuresis • High protein formula
Nursing diagnosis • Imbalance nutrition: less than body requirements • Weight monitoring to make caloric adjustment • Progress slowly to avoid gastric distention • Gradually add high calorie foods to maintain weight • Impaired skin integrity related to enzymatic action of gastric juices • Assess skin daily for signs & symptoms of irritation • Apply protective skin barrier • Strict handwashing • Patient & family teaching
Nursing diagnosis • Risk for aspiration • Positioning • Aspirate gastric contents before feeding • Disturbed body image related to presence of feeding tube • Encourage expression of feelings • Acknowledge patient fears • Provide correct information
Nursing diagnosis • Risk for deficient fluid volume/volume overload • Monitor mucous membranes & skin turgor, VS, I/O • Provide adequate fluid intake • Reinstill gastric contents to prevent electrolyte losses • Ineffective therapeutic regimen management • Give detailed information and return demonstration techniques to validate learning
Legal & Ethical Issues • Withholding food & fluids-what happens if clients are not able to make decisions or make their wishes known???? • Review what is known about tube feedings especially risks & benefits • Review medical facts about the client • Obtain the opinion of all stakeholders in this situation • Delay any action until consensus is achieved
Decompression Tubes • Occasionally, a tube can be used for acute treatment of active bleeding from esophageal or gastric varices. Two types are most common: • * The Sengstaken-Blakemore tube has a large balloon to compress the esophagus and a smaller one to anchor the tube and exert pressure against varices in the distal esophagus and the cardia of the stomach. It has three lumens-one each to inflate the balloons and one attached to suction to aspirate gastric contents. To suction secretions above the esophageal balloon, an additional tube, such as a Salem sump tube, is placed in the proximal esophagus. • * The Minnesota tube is similar to the Sengstaken-- Blakemore tube, but it also has an esophageal aspiration lumen that eliminates the need for an additional drainage tube.
Decompression Tubes • Gastric tubes-commonly used NG tubes that are placed for GI decompression or drainage.. • Salem sump- The Salem sump has two lumens, one for drainage and one for air. The drainage lumen is usually connected to low continuous suction. At times, however, higher levels may be needed. The air vent keeps the tube away from the stomach wall to prevent damage to the mucosa • The single-lumen Levin tube is typically connected to intermittent low suction for the same purpose.
Decompression Tubes • Intestinal Tubes mercury-filled balloon at the distal end. These tubes are rarely used today because the balloon could rupture and leak mercury. The newer Andersen tube, with a pre-weighted tungsten tip, is a safer option • Miller Abbot tube-A long 10’ (3 m) double-channel intestinal tube. Inserted through a nostril, the tube is passed through the stomach into the small intestine. Used for sampling gastrointestinal fluid or for therapeutic aspiration to relieve intestinal distension. • Cantor tube- 10’ single-lumen tube with a suction port in the lumen to aspirate contents • Harris Tube- short around 6’single lumen also to relieve distention, Y end allows lavage of intestinal tract • Dennis tube-10’ 3 lumen: irrigation, drainage & balloon inflation