Download
1 / 43
440 likes | 791 Vues
Drugs Used in Treatment of Malaria. Malaria is an infectious disease of humans caused by eukaryotic Sporozoal protozoon of the genus Plasmodium . It is widespread in tropical and subtropical regions, including parts of the Americas, Asia, and most of Africa.

E N D
Drugs Used in Treatment of Malaria • Malaria is an infectious disease of humans caused by eukaryotic Sporozoalprotozoon of the genus Plasmodium. • It is widespread in tropical and subtropical regions, including parts of the Americas, Asia, and most of Africa. • The disease results from the multiplication of malaria parasites within RBCs. • Malaria remains the world's most devastating human parasitic infection. Malaria affects over 40% of the world's population. WHO, estimates that there are 300 - 500 million cases of malaria annually worldwide, • 1-3 million died annually, ~90% of them occur among children under five years of age.
Anti-malarial drugs Anti-malaria drugs (cont’d) • Four species of Plasmodium can infect and be transmitted by humans. Severe disease is largely caused by P. falciparumwhich is responsible for about 90% of the deaths from malaria. • Malaria caused by P. vivax, P. ovale and P. malariaeis generally a milder disease that is rarely fatal. • A newly discovered fifth species, P. knowlesi, causes malaria in monkeys but can also infect humans. • P. falciparum accounts for 90% of deaths due to malaria and vivax is the most widely spread species because it exists in both temperate and tropical climates. • Malaria kills in one year what AIDS kills in 15 years. For every death due to HIV/AIDS there are about 50 deaths due to malaria. To add to the problem is the increasing drug resistance to the established drug. • The malaria life cycle is a complex system with both sexual and asexual aspects .
Anti-malarial drugs Pathogenesis: • The disease is transmitted to human via biting from the insect vector is the female Anopheles spp. mosquitoes, which breeds in stagnant water, and the disease it spreads is one of the major killers on our planet. • In plasmodium life cycle, man represents the (secondary) hosts, while female mosquito represents the definitive (primary) host. Only female mosquitoes feed on blood while male mosquitoes feed on plant nectar, thus males do not transmit the disease. • Plasmodium has a complex life cycle that part of it happened within the mosquito body and the rest of it happened within the human body
Anti-giardiasisdrugs Pathogenesis (cont’d): • The life cycle of all species that infect humans is basically the same. • The part of the life cycle in the mosquito is called “sporogenic cycle”.It is exogenous phaseduring which the parasite multiplies to give sporozoites(infective stage) and it includes both sexual and asexual forms of multiplication . • There is also an endogenous asexual phase that takes place in the vertebrate or human host that is called “schizogenic cycle”. • This phase includes the parasite development that takes place in the RBCs, called the “erythrocyticschizogeny” and the phase that takes place in the parencymal cells in the liver, called the “pre-erythrocyticschizogeny”. • The exo-erthrocytic phase is also called the tissue cycle.
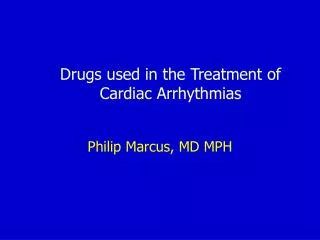
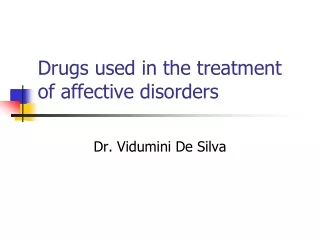
Anti-malarial drugs Plasmodium Spp life cycle Pre-erythrocytic cycle Schizogonic cycle Sporogonic cycle Erythrocytic cycle
Anti-giardiasisdrugs Pathogenesis (cont’d): Human pre-erythrocyticschizogony • Sporozoites are infective forms that present in the salivary gland of female anopheles mosquito. After bite of infected mosquito sporozoites are introduced into human blood circulation. • Sprozoites undergo developemtnal phase in the liver paranchymal cells. Sprozoites become in shape and multiple nuclear divisions develop to Schizonts(pre-erythrocytic stage of plasmodium). • On maturation Liver cells ruputure and schizonts liberate merozoites(erythrocytic stage of plasmodium)into blood stream. • A Schizont contains 20,000 – 50,000 merozoites.
Anti-giardiasisdrugs Pathogenesis (cont’d): Human pre-erythrocyticschizogony • Period of Pre-erythrocytic cycle: on average it take 6-16 days post infection for different types of plasmodium to complete the pre-erythrocytic cycle (P. vivax: 8 days, P. falciparum : 6 days, P. malariae : 13 – 16 days and P. ovale9 days). • In certain forms of malaria (P. vivax, P. ovale) some sporozoites entering the liver cells form hypnozoites, or dormant 'sleeping' forms of the parasite, which can be reactivated months or years later to continue an exo-erythrocyticcycle of multiplication.
Anti-giardiasisdrugs Pathogenesis (cont’d): Human erythrocyticschizogony • The librated merozoits invade the RBCs. Following mitotic replication of its nucleus, the merozoit in the RBCs is termed a schizont. Another phase of multiplication results in the production of further merozoites, which are released when the red cell ruptures. • These merozoites then bind to and enter fresh red cells, and the erythrocytic cycle starts all over again. • During maturation within the red cell, the parasite remodels the host cell, inserting parasite proteins and phospholipids into the red cell membrane. The host's haemoglobin is digested and transported to the parasite's food vacuole, where it provides a source of amino acids. Free haem, which would be toxic to the plasmodium, is rendered harmless by polymerisation to haemozoin. • Some antimalarial drugs act by inhibiting the haem polymerase enzyme responsible for this step.
Anti-giardiasisdrugs Pathogenesis (cont’d): Human erythrocyticschizogony • Typical symptoms of malaria include fever, shivering, arthralgia (joint pain), vomiting, anemia (caused by hemolysis), hemoglobinuria, and convulsions. • The classic symptom of malaria is cyclical occurrence of sudden coldness and shivering followed by rigor and then fever (may exceed 40C) and sweating lasting 4-8 hours. • These stages of malaria symptoms recur at regular intervals corresponding with synchronous release of merozoites from RBC (48-72 hrs). Most of malarial parasites causing tertianmalaria ('every third day') .
Anti-giardiasisdrugs Pathogenesis (cont’d): Human erythrocyticschizogony • Some liberated merozoites from RBCs undergo another developmental process to form motile intracellular parasites termed trophozoites. • This tophozoites differentiate into Male and female gametocytes (gametogony). • Macrogametocytes also called female gametocytes while microgametocyte also called as male gametocytes
Anti-giardiasisdrugs Pathogenesis (cont’d): Human erythrocyticschizogony • Some liberated merozoites from RBCs undergo another developmental process to form motile intracellular parasites termed trophozoites. • This tophozoites differentiate into Male and female gametocytes (gametogony). • Macrogametocytes also called female gametocytes while microgametocyte also called as male gametocytes
Anti-giardiasisdrugs Pathogenesis (cont’d): Mosquito sporogony (Sexual cycle) • The mosquito becomes infected when it takes a blood meal from an infected human. • Once ingested, the parasite gametocytes will further differentiate into male or female gametes. and then fuse (sexual reproduction) in the mosquito's gut. This produces an a zygote(ookinete) that penetrates the gut lining and produces an oocyst in the gut wall. • When the oocyst ruptures, it releases sporozoites that migrate through the mosquito's body to the salivary glands, where they are then ready to infect a new human host. • Can Malaria parasites also be transmitted by blood transfusions? Why?
Anti-malarial drugs Pathogenesis (cont’d): • The periodic episodes of fever that characterise malaria result from the synchronised rupture of infected RBCs with release of merozoites ,cell debris and other substances like inflammatory cytokines . • The rise in temperature is associated with a rise in the plasma concentration of TNF-α. • Recurence of malaria is likely to occur after treatment for three reasons. 1- Recrudescence occurs when parasites are not cleared by treatment, 2- Reinfection with new infection established from a separate infective mosquito bite; both can occur with any malaria parasite species. 3- Relapse is specific to P. vivax and P. ovale and involves re-emergence of blood-stage parasites from latent parasites (hypnozoites) in the liver. (exoerythrocytic cycle) after an interval of weeks or months to start the infection again.
Anti-malarial drugs Treatment of malaria: • The best way to eliminate malaria is to avoid the disease in the first place by eradicate the vector (Anopheles mosquito) in addition to use the antimalarial drugs (drugs which are used for prophylaxis, treatment and in the prevention for malaria), are also called antimalarials. • Several classes of antimalarial drugs are available . antimalarial drugs are classified in terms of the action against the different stages of the life cycle of the parasite. • Drugs used to treat the acute attack of malaria act on the parasites in the blood (blood schizonticides)e.g. quinine , mefloquine, chloroquine, halofantrine,sulfones, pyrimethamine, and artemether. Combinations of these agents are frequently used. Some antibiotics, such as clindamycin, tetracycline and doxycycline have proved useful when combined with the above agents. They act on the erythrocytic forms of the plasmodium. In infections with P. falciparum or P. malariae, which have no exoerythrocytic stage, these drugs effect a cure; with P. vivax or P. ovale, the drugs suppress the actual attack, but exoerythrocytic forms can re-emerge later to cause relapses.
Anti-malarial drugs Treatment of malaria (cont’d): • Drugs used for radical cure are active against parasites in the liver(tissue schizonticides). These agents’ effect a 'radical' (in the sense of striking at the root of the infection) cure by acting on the parasites in the liver e.g. primaquine and tafenoquine. • Drugs act on gametocytes and prevent transmissionby the mosquito (gametocides) and thus preventing the increase of the human reservoir of the disease e.g. primaquine, proguanil and pyrimethamine .
Anti-malarial drugs Treatment of malaria (cont’d): - Drugs used for chemoprophylaxis act on merozoites emerging from liver cells at the end of the pre-erythrocytic stage (causal prophylactic drugs).They block the link between the preerythrocytic stage and the erythrocytic stage, and thus prevent the development of malarial attacks. Chemoprophylactic agents are mostly given to individuals who intend travelling to an area where malaria is endemic. Administration should start 1 week before entering the area and should be continued throughout the stay and for at least a month afterwards. e.g. chloroquine, mefloquine, proguanil, dapsone and doxycycline. They are often used in combinations.
Anti-malarial drugs “causal prophylactics” “Tissue schizonticides” “Gametocides” “Blood schizonticides”
Anti-malarial drugs Major Anti-malarial Drugs
Anti-malarial drugs Antimalarials(1) 4-aminoquinoline drivatiives • Chloroquine and amodiaquine are synthetic 4-aminoquinoline drs.Chloroquine is formulated mainly as the phosphate salt for oral use. • It is effective against the erythrocytic forms (blood schizonticides) of all four plasmodial species (if sensitive to the drug), but it does not have any effect on sporozoites, tissue schizonts, hypnozoites or gametocytes. • It is considered a drug of choice in treatment of acute attack even resistance against chloroquine is a growing problem in most parts of the world especially of P. falciparumand P. vivax . • Chloroquine is also used as antirheumatoid, drug. Chloroquine
Anti-malarial drugs Chloroquine (cont’d) Mechanism of action • It is uncharged at neutral pH of the blood and can therefore diffuse freely into the parasite lysosome. At the acid pH of the lysosome, it is converted to a protonated, membrane- impermeable form and is 'trapped' inside the parasite. chloroquine acts mainly by inhibition of plasmpesin, the enzyme involved in haem disposal and preventing digestion of haemoglobinby the parasite and thus reducing the supply of amino acids necessary for parasite viability. It also inhibits haem polymerase that polymerises toxic free haem to haemozoin rendering it harmless to the parasite. • Resistance appears to result from enhanced efflux of the drug from parasitic vesicles as a result of mutations in plasmodia transporter genes
Anti-malarial drugs Chloroquine (cont’d) Pharmacokinetics: • Chloroquine is generally administered orally, but in severe cases, like falciparum malaria, may be treated by IV infusion or frequent small doses IM or SC. it is completely absorbed from GIT, extensively distributed throughout the tissues and concentrated in parasitised RBCS. Release from tissues and infected erythrocytes is slow. The drug is metabolized in the liver and excreted in the urine, (70% unchanged). Elimination is slow, half-life of 50 hours, and a residue persists for weeks or months. Adverse effects • Nausea and vomiting, loss of appetite, dizziness, drowsness and blurring of vision, headach, and urticaria are the most common unwanted effects. Bolus intravenous injections can cause cardiac dysrhythmias and postural hypotension. • It is not assigned by FDA for its safety during pregnancy, but it is the drug of choice for the prophylaxis and treatment of sensitive malaria species during pregnancy without evidence of fetal harm. • Amodiaquine has high risk of toxicity associated with prolonged administration for prophylaxis. The most serious adverse effects of amodiaquine are agranulocytosis and hepatotoxicity.
Anti-malarial drugs (2) 4-methanolquinolines a. Quinine and Quinidine: • Quinine is an alkaloid derived from the bark of Cinchona tree. They act as blood schizonticidal drugs effective against the erythrocytic forms of all four species of plasmodium. It has no effect on preerythrocytic and exoerythrocytic forms or on the gametocytes of parasite. Quinine • It interferes with heme polymerization, resulting in death of the erythrocytic form of the plasmodial parasite. • With the emergence and spread of chloroquine resistance, quinine is now the main chemotherapeutic agent for P. falciparum in many endemic regions. • Other pharmacological actions on host tissue include a depressant action on the heart, a mild oxytocic effect on the uterus in pregnancy, a slight blocking action on the neuromuscular junction and a weak antipyretic effect.
Anti-malarial drugs Quinine (cont’d) Pharmacokinetics: • Quinine is usually given orally and it is well absorbed, but it can also be given by slow IV infusion or I.M. for severe P. falciparum infections and in patients who are vomiting also for initiation of the medication. Quinidine is given only by I.V. route • The half-life of the drug is 10 hours; it is metabolized in the liver and the metabolites are excreted in the urine within about 24 hours. Alkalinization of the urine decreases its excretion. Adverse effects • Quinine has a bitter taste and is irritant to the gastric mucosa. • The major adverse effect of quinine is cinchonism’ that characterized by nausea, vomiting, dizziness, tinnitus, headache and blurring of vision. Excessive plasma levels of quinine can result in hypotension, cardiac dysrhythmias and severe CNS disturbances such as delirium and coma. These effects are observed to some extent in all patients receiving treatment and typically resolve with cessation of the medication. • Quinine can stimulate insulin release. Patients may have hypoglycemia. • Less commonly, hypersensitivity reaction with bronchospasm and cutaneous manifestations, such as flushing and urticaria, may occur. • Mostly given in combination with other blood schizonticidal drugs like pyrimethamine, dapsone or sulfadoxine. And antibiotic (eg, tetracycline, doxycycline or clindamycin
Anti-malarial drugs (2) 4-methanolquinolines (cont’d) b. Mefloquine: • Mefloquine is a synthetic analogue of quinine. That acts as blood schizonticidal compound. • active especially against chloroquine-resistant P. falciparum and P. vivax . • It has no effect on hepatic forms of the parasites, so treatment of P. vivaxand P. ovale infections should be followed by a course of primaquine to eradicate the hypnozoites. • The antiparasite action is associated with; inhibition of the haem polymerase. • Resistance has occurred in P. falciparum in some areas-particularly in South-east Asia-and is thought to be caused, by increased expression of pfmdr1drug efflux transporter in the parasite’s digestive vacules. Mefloquine (Lariam)
Anti-malarial drugs Mefloquine (cont’d) Pharmacokinetics: • Mefloquine is given orally and is rapidly absorbed. It has a slow onset of action and a very long plasma half-life (up to 4weeks), which may be the result of enterohepatic cycling or tissue storage. • Mefloquine is metabolized primarily through the liver. Execretion mainly in bile 95% and urine 5%. Elimination of mefloquine in anyone with impaired liver function may be prolonged, resulting in higher plasma levels and an increased risk of adverse reactions. Adverse effects • GIT disturbances,minimal cardiac arrythmia and transient CNS symptoms like dizziness, confusion, dysphoria and insomnia can occur. • The drug is contraindicated to be used in those with a previous history of seizures or a recent history of psychiatric disorders including anxiety, hallucinations, depression, and suicidal ideations. • Mefloquine users may experience sleep disturbances, including strange dreams and insomnia. • Mefloquine-induced pneumonitis is an infrequently reported but serious adverse event in the setting of both prophylactic and therapeutic use. One-third of the patients improved following treatment with corticosteroids, and most patients fully recovered upon discontinuation of the drug. • Little is known about mefloquineteratogenic potential, so the WHO approved the use of drug in the 2nd and 3rd trimester of pregnancy. Women should however not become pregnant and should use effective birth control while taking mefloquine and within 3 months of stopping the drug, because of its long half-life and uncertainty about its teratogenic effects.It may be used during breastfeeding, though the drug appears in breast milk in low concentrations. • The combination of mefloquine plus artesunate appears to be effective in most regions.
Anti-malarial drugs (3) Phenanthrene-methanols • Lumefantrine , and Halofantrine are blood schizonticidal drugs active against all species of malarial parasite, including multidrug-resistant strains of P. falciparum that are resistant to many antimalarials like chloroquine, quinine, and pyrimethamine . Cross-resistance between halofantrine and mefloquine has been reported • They have similarity in structure to the 4-methanolquinolines • In vitro studies suggest that they bind to and inactivate plasmpesins, a haemoglobin degrading enzymes unique to the malarial parasites. Halofantrine (Halfan)
Anti-malarial drugs Halofantrine (cont’d) Pharmacokinetics: • Halofantrine is given orally. It is slowly absorbed, with a peak plasma concentration achieved approximately 4-6 hours after ingestion (absorption is substantially increased up to three- to fourfold when taken with a high fat meal). The half-life is 1-2 days, although its main metabolite (desbutylhalofantrine), which has equal potency, has a half-life of 3-5 days. Elimination is in the faeces. • Lumefantrine is given orally with longer half-life of 3 to 6 days. It is used with its usual partner drug “artemether” in a widely used fixed-dose combination. Adverse effects: • Abdominal pain, GIT disturbances, headache, skin rashes and cough may occur. • Halofantrine can produce cardiac arrhythmia particularly if given with other drugs like mefloquine, and it should be used with caution in patients with a history of dysrhythmia. It may cause sudden cardiac arrest in most severe cases. • Because of such cardiotoxicity, halofantrine use is now limited to treat infections caused by resistant organisms. • Lumefantrine is well tolerated, with rare mild adverse reactions such as diarrhea, nausea, abdominal pain, and vomiting.
Anti-malarial drugs (4) 8-aminoquinoline drivatives • Primaquine the only 8-aminoquinoline dr. in clinical use. • Etaquineand tafenoquineare more active primiqune analogues with prolonged duration and less side effects are still in the pre-clinical trials. • Primaquine and its related drugs are active against the liver forms of the parasite (tissue schizonticides), It can produce a radical cure of those forms of malaria in which the parasites have a dormant stage (hypnozoites) in the liver Largely it is used to prevent relapse of P. ovale and P. vivax malaria Primaquine
Anti-malarial drugs primaquine (cont’d) • Primaquine does not affect sporozoites and erythrocytic stage of the parasite. However, it has a gametocidalaction and is the most effective antimalarial drug for preventing transmission of the disease in all four species of plasmodia. • It is almost invariably used in combination with another drug, usually chloroquine. Resistance to primaquine is rare. Mechanism of action • Metabolites of primaquine are believed to act as oxidants that are responsible for the schizonticidal action
Anti-malarial drugs Primaquine (cont’d) Pharmacokinetics: • Primaquine is well absorbed on oral administration and is not concentrated in tissues. It is rapidly metabolized to many compounds, the major one being the deaminated drug. very little drug is present in the body after 10-12 hours. The half-life is 3-6 hours. Tafenoquine is broken down much more slowly and therefore has the advantage that it can be given on a weekly basis. Metabolites are execreted in the urine Adverse effects • Primaquine has few unwanted effects in most patients, but some symptoms like GIT upset headache, visual disturbances and itching. Large doses may cause methaemoglobinaemia with cyanosis.
Anti-malarial drugs Primaquine (cont’d) • Primaquine-associtedmethaemoglobinaemia is always less sever and self-limiting in most caseas. • Dangerous levels of methemoglobinemia only occur in patients G-6-PD deficiency (people of African or Mediterranean descent). The oxidant metabolic derivatives of primaquine. As a consequence, the metabolic functions of the red cells are impaired and haemolysis occurs (hemolytic anemia ). • Primaquine should not be administered to anyone with G-6-PD deficiency because there can be a severe reaction with hemolytic anemia. • Primaquine is contraindicated in pregnancy and breastfeeding.
Anti-malarial drugs (5) Antimalarialantifolates (DHPS) (DHFR) • Mostly used in combination with each other to give synergistic action.
Anti-malarial drugs (5) Antifolates (cont’d) a. Pyrimethamine : • It is a 2,4-diaminopyrimidine (similar in structure to trimethoprim). • It acts by interfering with DNA and RNA synthesis through disturbing tetrahydrofolic acid synthesis, by inhibiting the enzyme DHFR. It has a greater affinity for the plasmodial enzyme than for the human enzyme. • It is active against the erythrocytic forms of the parasite. Also, it has a gametocidalaction. • Pyrimethamine is given orally and is well, absorbed. It has a plasma half-life of 4 days, and effective 'suppressive' plasma concentrations may last for 14 days; it is taken once a week. Pyrimethamine (Daraprim) • The most common unwanted effects associated with pyrimethamine therapy include GI upset and headache. Mild bone marrow suppression may occur with blood changes (leukopenia, thrombocytopenia & hemolytic anemia with hematourea), hemolysis is more pronounced in patients with G6PD deficiency. Allergic reactions (rashes & hives) may also reported. • In high doses, it may inhibit mammalian DHFR and cause a megaloblasticanaemia; folic acid supplements should be given if this drug is used during pregnancy.
Anti-malarial drugs Pyrimethamine (cont’d) • Pyrimethamine is used only in combination with either artesenuate, dapsoneor a sulfonamide. • Dapsoneis a sulfone drug mostly used in combination with pyrimethamine in the treatment of malaria. • Sulfadoxineis an ultra-long-lasting sulfonamide often used in combination with pyrimethamine to treat or prevent malarial infection. • The combination is considered to be more effective in treating malaria caused by multidrug-resistant P. falciparum • Also, combination is indicated in the absence of a species-specific diagnosis. • Resistance to pyrimethamine mono-or combined therapy like sulfadoxine-pyrimethamine occurs usually via mutations in the target enzymes DHFR and DHPS. P. falciparum resistance to sulfadoxine-pyrimethamine is widespread in most malaria-endemic regions. Dapson Sulfadoxine
Anti-malarial drugs (5) Antifolates (cont’d) b. Proguanil: • It is chemically related to biguanides. • Same like pyrimethamine, it interferes with nucleic acid synthesis. • It is active against the erythrocytic forms of the parasite . Proguanil also has an additional effect on the initial hepatic stage but not on the hypnozoites of P. vivax and P. ovale. It is effective causal prophylactic drug. Proguanil (Paludrine) • It is given orally. Proguanil is a prodrug and is metabolised in the liver to its active form, cycloguanil, which is excreted mainly in the urine. It is well absorbed from GIT and its half-life is ~16 hours. It must be taken daily. • Proguanil is usually taken in combination with another anti-malarial drug such as chloroquine or atovaquone (e.g., in the drug Malarone) to treat multidrug-resistant strains of P. falciparumand P. vivax. • Proguanil has few unwanted effects ; abdominal pain, vomiting, diarrhea, headache ,mild hypersensitivity effects (pruritis), and some feelings of irritability and mild anxiety (drug should be avoided to be used in those with a previous history of psychiatric disorders including anxiety, and hallucinations.
Anti-malarial drugs (6) Hydroxynaphthoquinone derivatives Atovaquone Atovaquone: • It is used for the treatment of malaria and can prevent its development. • It acts mainly as ubiquinone inactive analogue to inhibit the parasite's mitochondrial electron transport chain. • Atovaquone is active against both tissue and erythrocyticparsitic stages, allowing chemoprophylaxis to be discontinued only 1 week after the end of exposure • Atovaquone is usually used in combination with the antifolate drug proguanil, because they act together to cause a synergistic antimalarial effect. They interferes with two separate pathways. • In addition, proguanil appears to act via a direct mechanism outside the folate pathway, enhancing atovaquone's mitochondrial membrane toxicity that give marvelous outcomes for this particular pair of drugs. Usually used in combination with Progunil (Malarone)
Anti-malarial drugs (6) Atovaquone (cont’d) Pharmacokinetics: • Atovaquone is administered orally. Its bioavailability is low and irregular, but absorption is increased by fatty food. The drug is heavily protein-bound and has a half-life of 2–3 days. • Most of the drug is eliminated unchanged in the feces. Adverse effects: • When combined with proguanil, atavaquone is highly effective and well tolerated. Few side effects of such combination have been reported, but abdominal pain, nausea , vomiting , and diarrhea can occur. • Pregnant or breast-feeding women should not take atovaquone. • Resistance to atovaquonemonotherapy is rapid and results from a single point mutation in the mitochondrial gene encodes cytochromeb, while resistance to combined treatment with atovaquone and proguanilis less common.
Anti-malarial drugs (7) Artemisnins • Artemisinin is naturally isolated compound from leaves of chineese herb; Artemisia annua. Because artemisinin itself has poor bioavailability that limit its effectiveness, semi-synthetic derivatives of artemisinin, including Artesunate, artemether, and arteether, have been developed . Artemisnin • Artmisinins have the fastest parasite clearance times of all current antimalarial drugs . They are fast-acting blood schizonticide effective in treating the acute attack of malaria (including multidrug-resistant falciparum malaria). They also possess gametocidal activity.
Anti-malarial drugs (7) Artemisnins (cont’d) • All artemisinins used today are prodrugs of the biologically active metabolite dihydroartemisinin, which is concentrated in parasitised RBCs. • The detailed mechanism of action is not clear, but one theory states that when the parasite that causes malaria infects a red blood cell, it consumes hemoglobin within its digestive vacuole, liberating free heme. Artemisinins appear to act by binding heme’s iron. The iron reduces the peroxide bonds in artemisinin generating high-valent iron-oxo species, resulting in a cascade of reactions that produce free radicals (ROS) which damage the parasite’s multiple targets including proteins, nucleic acids and others leading to its death.
Anti-malarial drugs (7) Artemisnins (cont’d) • Artemisinin and its derivatives are also potent anthelmintics especially in treatment of the human blood flukes infections, schistosomiasis, which are the second most prevalent parasitic infections, after malaria. • Artemisinin and related compounds are tested as anticancer drugs. • Use of the drug by itself as a monotherapy is clearly discouraged by the WHO as there have been signs that malarial parasites are developing resistance to the drug. Instead combined therapy including artemisinins (like artemether + lumefantrineOR Pyrimethamine + artesenuate).
Anti-malarial drugs (7) Artemisnins (cont’d) Pharmacokinetics: • Artemisinin can be given orally, IM or rectally by suppository. Artemether , artesunateand artether are given either orally , rectally, IM, or IV. • They are rapidly absorbed and widely distributed, and are converted in the liver to the active metabolite dihydroartemisinin. • The half-life of artemisinin is about 4 hours, of artesunate 45 minutes and of artemether 4-11 hours. Adverse effects: • Few adverse effects have been reported with artrmisinin and related compounds. • For example, transient bradycardiaespecially with IV infusion, decrease in blood neutrophil count, and brief episodes of fever. Transient neurological abnormalities have been reported, including nystagmus and disturbances in balance these effects resolved without lasting sequelae as theray is stopped.
Anti-malarial drugs (8) Antibiotics • Tetracycline, doxycycline, and clindamycin target prokaryotic protein synthesis. In malaria parasites, these drugs appear to target the apicoplast, a vital organelle in plasmodial cell • Antimicrobials have relatively slow blood schizonticidal effects because they exert their toxic effects in the subsequent cycle of cell division . They are typically paired with fast-acting antimalarials (usually quinine and chloroquine). • Doxycycline has a longer half life than tetracycline so is used more commonly. • Resistance has not been detected to tetracycline, doxycycline or clindamycin. • Adverse effects are common with the tetracyclines and interfere with adherence. GI discomfort and candidiasissuperinfection are the most frequent complaints. • Doxycycline therapy also poses a risk of esophageal ulceration and photosensitivity especially if utilizedfor prolonged time in causal prophylaxis. • Tetracyclines should not be given to pregnant women or children less than 8 years old because of the risk of deposition in growing bones and teeth. • Clindamycin is the preferred alternative in these groups.