Initial Therapy
Initial Therapy. Anti-ischemic and Analgesic therapy Anti-platelet therapy Anti-coagulant therapy. Management of UA/NSTEMI. Management Before UA/NSTEMI and Onset of UA/NSTEMI Initial Evaluation and Management of UA/NSTEMI Early Hospital Care


Initial Therapy
E N D
Presentation Transcript
Initial Therapy • Anti-ischemic and Analgesic therapy • Anti-platelet therapy • Anti-coagulant therapy
Management of UA/NSTEMI Management Before UA/NSTEMI and Onset of UA/NSTEMI Initial Evaluation and Management of UA/NSTEMI Early Hospital Care Select Management Strategy: Initial Invasive Versus Initial Conservative Strategy Initial Invasive Strategy Initial Conservative Strategy Revascularization and Late Hospital Care Coronary Revascularization Late Hospital Care, Hospital Discharge and Post-Hospital Discharge Care Long-Term Medical Therapy and Secondary Prevention Special Groups
Important Points in Hospital Care • Stress test before discharge for assessment of ischemia in initial conservative strategy. Must be free of resting ischemia or HF for 12-24h – Class I, C • If not classified as low risk, angiography should be performed – Class I, A • Fasting lipid panel within 24 hours – Class I, C • Statin regardless of baseline LDL-C pre-discharge • Echo or MUGA must be done if no plan for left ventriculography by angiogram – Class I, B
Initial Conservative Strategy: Early Hospital Care (1) • ASA; clopidogrel if intolerant (I, A) • Anticoagulant therapy should be added to antiplatelet therapy as soon as possible after presentation (I, A) • Enoxaparin or UFH (I, A) • Fondaparinux (I, B) • Enoxaparin or fondaparinux preferable (IIa, B) • Initiate clopidogrel, loading dose + maintenance dose (I, A) • Consider IV eptifibatide or tirofiban (IIb, B)
Initial Conservative Strategy: Early Hospital Care (2) • If LVEF is < 0.40, it is reasonable to perform diagnostic angiography (IIa, B) • A stress test should be performed for assessment of ischemia (I, B) • If the patient is classified as not as low risk, diagnostic angiography should be performed (I, A) • Measurement of BNP or NT-pro-BNP may be considered to supplement assessment of global risk in patients with suspected ACS (IIb, B)
Initial Conservative Strategy: Early Hospital Care (3) • Beta blocker therapy • Initiate oral therapy within first 24 hr unless HF, low-output state, increased risk for cardiogenic shock, or relative contraindications (I, B) • IV therapy for high blood pressure without contraindications (IIa, B) • IV therapy may be harmful with contraindications to beta blockade, signs of HF or low-output state, or other risk factors for cardiogenic shock (III, A)
Initial Conservative Strategy: Early Hospital Care (4) • Lipid management • Fasting lipid profile within 24 hr (I, C) • Statin (in absence of contraindications) should be given regardless of baseline LDL-C pre-discharge (I, A) • ACE inhibitor (oral) • Within 24 hr with pulmonary congestion or LVEF 40, in absence of hypotension (systolic blood pressure <100 mmHg or <30 mmHg below baseline) or known contraindications (I, A) • ARB if ACE intolerant (I, A) • Can be useful without pulmonary congestion or LVEF < 0.40 (IIa, B) • No IV ACE-I in first 24 hr because of increased risk of hypotension (III, B)
More Aggressive Long-Term Antiplatelet Therapy • Medical therapy without stenting • ASA 75-162 mg/d indefinitely (I, A) + • clopidogrel 75 mg/d, at least 1 mo (I, A), ideally up to 1 yr (I, B) • Bare metal stent • ASA 162-325 mg/d at least 1 mo, 75-162 mg/d indefinitely (I, A) + • clopidogrel 75 mg/d, at least 1 mo (I, A), ideally up to 1 yr (I, B) • Drug-eluting stent • ASA 162-325 mg/d at least 3 (sirolimus)-6 (paclitaxel) mo, 75-162 mg/d indefinitely (I, A) + • clopidogrel 75 mg/d at least 1 yr (I, B)
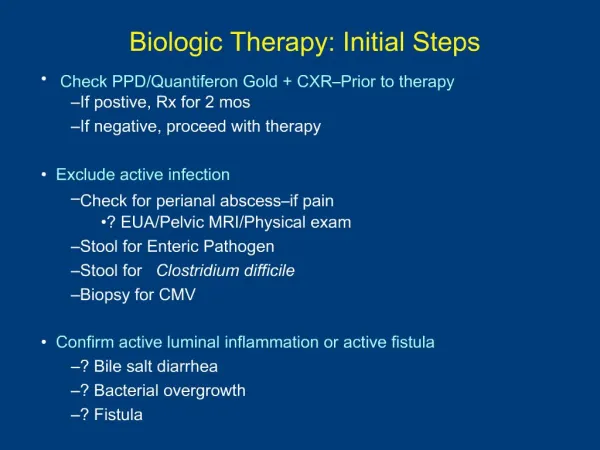
Treatment • Oxygen • Aspirin • Beta-blocker • Nitroglycerin • Morphine • Heparins, DTIs • IIb/IIIa inhibitors • Plavix • ACE/ARB • Aldosterone Blockade • Statins • Increases oxygen supply to ischemic tissue • Start at 4L/min • Use caution in COPD patients
Anti-ischemic and Analgesic Therapy • Bed/chair rest – Class I, C • O2 for SaO2 < 90%, respiratory distress, or hypoxemia – Class I, B • NTG 0.4 mg sl q 5 min x 3 doses, then gtt for ongoing ischemic discomfort – Class I, C • NTG iv within 48h for persistent ischemia, HF, or HTN. Should not preclude use of BB – Class I, B • Oral BB therapy within 24h without 1) HF, 2) low output, 3) risk of shock, 4) relative contraindications – Class I, B
Anti-ischemic and Analgesic Therapy • CCB (nondihydropyridine) if contraindication for BB in the absence of contraindications – Class I, B • ACE inhibitor for LVEF <0.40 and no hypotension (SBP <100 or <30 below baseline) – Class I, A • ARB if intolerant to ACE inhibitor – Class I, A • NSAIDS should be discontinued – Class I, C
Anti-Platelet Therapy • ASA – started immediately and continued indefinitely – Class I, A • Plavix – loading dose (300-600mg)* plus maintenance 75 mg if ASA intolerant – Class I, A • If h/o GIB, PPI plus anti-platelet therapy – Class I, B • GP IIB/IIIA therapy depends on strategy chosen (more on this later) * Risk/benefit to higher loading dose regimens is yet to be determined
Anti-Coagulant Therapy • Anticoagulant Therapy should be added to antiplatelet therapy as soon as possible after presentation • Choice of anticoagulant depends on the strategy chosen (more on this later)
Anticoagulants and Antiplatelets – Initial Invasive Strategy
Anticoagulants and Antiplatelets – Initial Conservative Strategy
Initial Invasive Strategy: Antiplatelet, Anticoagulant Therapy • Initiate anticoagulant therapy as soon as possible after presentation (I, A) • Enoxaparin or UFH (I, A) • Bivalirudin or fondaparinux (I, B) • Prior to angiography, initiate one (I, A) or both (IIa, B) • Clopidogrel • IV GP IIb/IIIa inhibitor Use both if: • Delay to angiography • High risk features • Early recurrent ischemic symptoms
Molecular Structure • Generic: clopidogrel bisulfate • Class: ADP-receptor antagonist • Molecular weight = 419.9
CLOPIDOGREL C ADP ADP Collagen thrombin TXA GPllb/llla (Fibrinogen receptor) Activation 2 ASA COX TXA 2 The activemetabolite exerts its antiplatelet effect by noncompetitiveinhibition of the platelet ADP receptor subtype P2Y12 Clopidogrel: Aninactive prodrug requires in vivo conversion in the liverby the cytochrome P450 (CYP) 3A4 enzyme system COX (cyclo-oxygenase) ADP (adenosine diphosphate) TXA2 (thromboxane A2)
The thienopyridine clopidogrel A prodrug that needs to bemetabolized by cytochrome P450 (CYP) to 2-oxo-clopidogrel, an intermediatemetabolite that is further hydrolyzed to the active thiol metaboliteof clopidogrel
The thienopyridine clopidogrel The active metabolite irreversibly binds tothe P2Y12 receptor The major circulatingmetabolite of clopidogrel is a carboxylic acid derivate thatcompletely lacks antiaggregatoryactivity
Pharmacology of Clopidogrel Absorption (oral): rapid Not affected by food or antacids Metabolism: rapid and extensive hepatic metabolism
Pharmacology of Clopidogrel Half-life: 8 hours (but has an irreversible effect on platelets, with a lifespan of approximately 7–10 days) Excretion: 50% in urine and 46% in feces, after 5 days
Side Effect Of Clopidogrel • Rash, or manifestations of a hypersensitivity reaction to clopidogrel
Side Effect Of Clopidogrel Management include: • Clopidogrel desensitization • Treatment with antihistamines and corticosteroid cream • Switching to ticlopidine.
GP IIb/IIIa inhibitors Several GP IIb/IIIa inhibitors exist: • abciximab (ReoPro) • eptifibatide (Integrilin) • tirofiban (Aggrastat)
New Long-Term Antithrombotic Therapy at Hospital Discharge after UA/NSTEMI UA/NSTEMI Patient Groups at Discharge Medical Therapy without Stent Bare Metal Stent Group Drug Eluting Stent Group ASA 162 to 325 mg/d for at least 3 to 6 months, then 75 to 162 mg/d indefinitely (Class I, LOE: A) & Clopidogrel 75 mg/d for at least 1 year (Class I, LOE: B) ASA 75 to 162 mg/d indefinitely (Class I, LOE: A) & Clopidogrel 75 mg/d at least 1 month (Class I, LOE: A) and up to 1 year (Class I, LOE: B) ASA 162 to 325 mg/d for at least 1 month, then 75 to 162 mg/d indefinitely (Class I, LOE: A) & Clopidogrel 75 mg/d for at least 1 month and up to 1 year (Class I, LOE:B) Indication for Anticoagulation? Yes No Add: Warfarin (INR 2.0 to 2.5) (Class IIb, LOE: B) Continue with dual antiplatelet therapy as above Anderson JL, et al. J Am Coll Cardiol 2007;50:e1–e157, Figure 11. INR = international normalized ratio; LOE = level of evidence.