Download
1 / 38
420 likes | 3.1k Vues
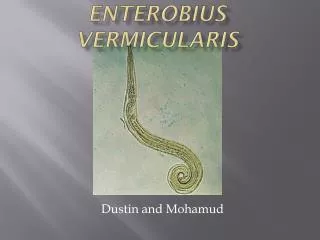
ENTEROBIUS VERMICULARIS. Also called pin worm ,thread worm or seat worm. First described by Leuckart in 1865. E.vermicularis is the only species . Habitat—adult worm remain attached to large intestine (cecum .appendix and adjacent part of colon ) by their mouth. Epidemiology.

E N D
Also called pin worm ,thread worm or seat worm. • First described by Leuckart in 1865. • E.vermicularis is the only species . • Habitat—adult worm remain attached to large intestine (cecum .appendix and adjacent part of colon ) by their mouth
Epidemiology • Global prevalence in human -290 million infected . • Prevalence is maximum in school children between age of 5 and 15 years . • People carry infection for years due to auto infection . • Factors –over crowding and poor personal care .
Morphology • Adult worm-small white and thread like . • Adult worm bears a wing like expansion of cuticle near the anterior end called cervical alae. • Posterior end of esophagus dilated to form a glandular bulb-the double bulb esophagus. • Male smaller 2-5mm x 0.1mm and posterior 1/3rd is tightly curved and bears a copulatory bursa . Male die soon after fertilisation. • Female 8-13mm x 0.3mm and posterior 1/3 tapering, straight pointed and look like pin.
Eggs • Oval or planoconvex . • 50 to 60 u long and 20 to30 u wide . • Surrounded by double layered egg shell. • Non bile stained ,floats in saturated solution of salt . • Embryonated when passed fresh, contain a tadpole larva
Host—only human • Mode of transmission—acquire infection by ingestion of embryonated egg containing larva by • Ingestion of eggs contaminated with fingers due to inadequate hand washing or nail biting. • Autoinfection- endogenous autoinfection by retrograde migration of larva hatched from the egg in perianal skin. • Exogenous autoinfection-eggs cause intense irritation of perianal skin and scraping of area leads to contaminated finger and rarely inhalation .
Development in man • Eggs containing fully developed larvae hatch out releasing larvae in cecum and develop into adult worm . • Female mature in 1 month ,after fertilization male die • Gravid female fully filled with eggs migrate to large intestine and start laying eggs on perianal skin and lay 2000 eggs/day . • Eggs are infective to man . • Female live for 2 months but because of auto infection cycle repeat .
Pathogenicity and clinical features • Asymptomatic • Symptomatic---Perianal pruritis due to nocturnal migration of female Excoriation of perianal skin and bacterial super infection. Abdominal pain and weight loss . • Migration of worm- worm may invade female genital tract causing vulvo vaginitis and pelvic and peritoneal granuloma .Other sites being urinary tract, peritoneal cavity ,lungs and liver
Lab diagnosis • As female lay eggs in perianal area eggs rarely detected in stool examination .So eggs deposited are collected by cellophane tape or its modification NIH swab • Cellophane tape method—apply clear cellulose acetate tape to perianal area in morning before child goes for bath • The tape is applied on the clear glass slide and observed under microscope for eggs
NIH swab method • Devised by National institute of health USA . • Has a glass rod attached to a cellophane tape by a rubber band . • Other end of it is fixed by a rubber stopper and kept in a test tube . • Cellophane part rolled over perineal and perianal skin to collect sample . • The tape transferred to a slide examined under microscope • Adult female may be rarely seen in feces or crawling in perianal skin
Treatment—Albendazole or Mebendazole or Pyrantal pamoate and should be repeated after two weeks and treat household members also • Prevention—improve personal hygiene
Strongyloidesstercoralis • Also known as military worm • Strogyloides belongs to super family Rhabditoidea and family Strongyloididae • It comprises of 53 species but human infection is only by S.stercoralis and S.fuelleborni .
Epidemiology • Found in hot humid tropical areas • Mostly in S.E . Asia , Sub saharan Africa and S . America • In western world it is found in immigrants, refugees , travellers and military personals.
Habitat • Parasitic female resides in human intestine (duodenum and jejunum ) where as free living female multiply in environment . • Male are always free living . Most believe that parasitic male does not occur .
Adult worm—only females seen in human intestine • Parasitic female 2-3 mm x 30-50 u and free living female 1 mm x 80 u . • Alimentary tract anterior portion is thicker bear mouth and three small lips, esophagus ( with posterior bulb and three esophageal glands ) followed by intestine and mid ventral anus . • Female reproductive organ consists of paired ovaries ,oviduct and uteri which joined to form vagina that leads to vulval opening
Free living male worms are slightly smaller have two spicules at the posterior end . • Other feature are similar to any trematodes
Eggs—eggs are conspicuous within gravid females arranged anteroposteriorly in a single row of 5 to 10 eggs in each uterus . • Oval and 50-70 u long . • Ovoviviparous ,i .e they immediatly hatch out to larvae
Larva • Four stages of larva L1 to L4 • LI-first stage – rhabditiform larva—eggs hatch to form L1 in human intestine .250 x 16 micron has buccal cavity , double bulb esophagus and large genital primordium . • It is the diagnostic form found in human feces . • L3 –filariform larva—in environment L1 moult twice toform L3 larva . 630 x 16 u .Has long cylindrical esophagus and a notched tail. • L3 larva is infective to human .
Life cycle • Host– human rarely domestic pets • L3 –filariform larva is infective • Mode of transmission—Penetration of skin by L3 with help of penetration . Autoinfection-internal autoinfection • Migratory phase—After penetration L3 enter subcutaneous small venules through venous circulation reach right heart and finally to lungs . • Here they enter alveolar space migrate to bronchi ,trachea and finally by swallowing sputum to GIT
Intestinal phase—L3 under go third moult to form L4 and reach small intestine and undergo final moult to become adult. • Adult male not found in human intestine . • Laying eggs-only female worms found buried in the intestinal mucosa . • They can directly lay eggs without fertilization (Parthenogenisis) . • Eggs hatch to liberate LI (rhab) larva into intestinal lumen and passed in feces .
Autoinfection---some times L3 larvae released in human intestine dont pass in feces but develop into filariform larva and penetrate intestinal wall or perianal skin enter venous circulation and reach lungs • Autoinfection is responsible for maintaining infection as long as 30-40 years and can cause disseminated infection .
Development in environment • In moist and warm soil L1 moult twice to form L3. • Then two type of development takes place (direct and indirect ) • Direct—L3 act as infective form and infect man through the penetration of skin . • Indirect form—L3 moult twice to develop into adult worm (male and female ) in environment . • Free living adult worms fertilize ,lay eggs that hatch out soon to L1 which moult twice to form infective L3 (filar )
Pathogenesis and clinical features • Affect due to migrating larva • Asymptomatic infection . • Rashes-recurrent maculopapular . • Cutaneous larva migrans-migrating larvae may produce pathagnamonic serpiginous urticarial rash called larva currens . • Pulmonary symptoms may be uncommon .
Affect due to worm and filariform larva • Mild to moderate worm load-epigastric pain nausea diarrhea nad blood loss . • Heavy larval load—Hyperinfection syndrome and disseminated strongyloidiasis syndrome
Lab investigation • Microscopy—the rhabditiform larva can be demonstrated in stool by direct microscopy . • Hook worm egg may hatch in stool releasing rhab larvae and has to be differenciated from that of Strongyloides • Entero test can be used • Desseminated strongyloides can be readily diagnosed by examination of stool sputum other body fluids and contains typically high number of filariform larvae
Stool culture—Freshly passed stool can be cultured L3 are formed within 2 days . • Culture techniques includes __Harada mori filter paper tube method ,Salt culture , Charcoal culture ,Baermann funnel and agr plate technique .
Serology • ELISA---when microscopy is negative • Luciferase immune precipitation—detect IgG • Molecular methods-detect strongyloid DNA in stool
Treatment—Ivermetrin 200mg/kg for two days • Prevention—Personal care and hygiene
S.fuelleborni---monkey and apes occationaly cause human infection • Swollen belly syndrome---diarrhea ,respiratory distress and protein loosing enteropathy lead to hypoalbuminaemia and edema
Answer these • Classify intestinal nematodes .Describe the life cycle ,pathogenesis and lab diagnosis of S.stercoralis ? • Short note on---E .vermicularis Hyperinfection syndrome NIH swab