Download
1 / 36
360 likes | 945 Vues
Profilassi di infezione HBV dopo puntura accidentale. Se operatore sanitario suscettibile (HBsAg e HBsAb negativo) somministrare preferibilmente entro le 24/ore immunoglobuline specifiche al dosaggio di 0,06ml/Kg

E N D
Profilassi di infezione HBV dopo puntura accidentale Se operatore sanitario suscettibile (HBsAg e HBsAb negativo) • somministrare preferibilmente entro le 24/ore immunoglobuline specifiche al dosaggio di 0,06ml/Kg • iniziare il ciclo vaccinale entro il 14o giorno dall'avvenuto contatto (possibilmente entro 96 ore) seguendo lo schema accelerato di somministrazione delle dosi 0,1,2 mesi e dose di rinforzo a distanza di 6-12 mesi dalla terza. Se l'operatore rifiuta la vaccinazione è consigliabile la somministrazione di una seconda dose di immunoglobuline specifiche dopo un mese
Profilassi di infezione HBV dopo puntura accidentale Operatore sanitario non suscettibile: • operatore sanitario vaccinato con ciclo completo e classificato come “responder”: nessun provvedimento • operatore sanitario vaccinato con ciclo completo e classificato come “non responder” o “low responder” con titolo HBsAb fra 10 e 100 o < 10 mUl/ml, valutare i casi singolarmente soprattutto in relazione al tempo intercorso dalla vaccinazione: può essere opportuno proporre una dose di richiamo di vaccino
Profilassi di infezione HBV dopo puntura accidentale Operatore sanitario la cui risposta al ciclo vaccinale non è nota: Valutare il tempo intercorso dalla vaccinazione e determinare titolo HBs-Ab: • se titolo HBsAb >100 mUl/ml: nessun provvedimento • se titolo HBsAb tra 10 e 100 mUl/ml: 1) valutare l'opportunità di proporre 1 dose di richiamo se titolo HBsAb < 10 mUl/ml: 1 dose di richiamo di vaccino • Se l'operatore sanitario risulta HBsAg positivo è da verificare nel pz fonte lo stato sierologico nei confronti del virus delta
SilentCirrhosis Resolution Resolution LiverCancer Death Long-termCarrier Cirrhosis Death 30 - 50 Years Progression of Hepatitis B Infection Short-termInfection Long-termHepatitis Cirrhosis
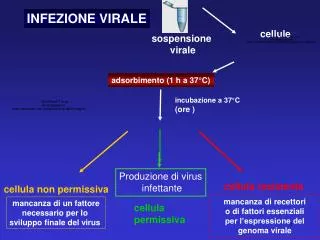
EPATITE VIRALE C • INCUBAZIONE: 15-160 gg(in media 50) • TRASMISSIONE: parenterale,sessuale,salivare • CONTAGIOSITA’ perenne nelle forme croniche • EVOLUZIONE 50-80% cronicizza ed evolve in cirrosi
Sono a rischio di contrarre l’epatite C ¨Tossicodipendenti ¨Lavoratori che possono venire a contatto con sangue umano ¨Pz in emodialisi ¨Pz trasfusi Possono essere a rischio Pz che hanno rapporti sessuali con diversi partners Conviventi di pz con epatite C
Oltre all'infezione post-trasfusionale, oggi per altro in netta diminuzione grazie ai test sierologici di screening sul sangue trasfuso, si prospettano altre vie di contagio sia di tipo parenterale che non, come i contatti tra i familiari, l'uso di farmaci o droghe per via E.V. utilizzando materiale non sterile, il contatto professionale, le infezioni ospedaliere, l'emodialisi e la convivenza in istituti, le cure dentarie. L'epatite C è attualmente la più frequente delle epatiti ed è responsabile di una percentuale ancora imprecisata di epatiti croniche; probabilmente è la causa della maggior parte delle cirrosi in passato definite criptogenetiche. E' una epatopatia ad evoluzione generalmente lenta, (Dal contatto alla cirrosi passano 10 anni, 15 dalla comparsa dell’epatocarcinoma) .discretamente tollerata dal paziente Il 33% può sviluppare una epatite cronica . Solo il 5% dei pazienti risulta sintomatico. Occorre quindi monitorizzare il paziente per lunghi periodi perchè le transaminasi (in particolare le alt ) possono avere ampie oscillazioni con picchi di citolisi o rimanere per lunghi periodi costantemente elevate (caso piu raro) .
EPATITI CRONICHE DEFINIZIONE infiammazione cronica del fegato che si protrae per almeno sei mesi senza remissione. Per fare diagnosi di epatopatia cronica dobbiamo controllare mensilmente le transaminasi ed osservare un alterazione che si protrae per almeno sei mesi consecutivi. L’alterazione delle transaminasi non è pero strettamente correlata con l’entità del danno e quindi, una volta fatta la diagnosi bisogna inviare il pz dallo specialista (per eventuale biopsia ed impostazione terapia con interferon)
100 acute HCV infections 20% recovery 80% persistent infections 80 patients 20 patients 40% variable progression 30% severe progressive hepatitis 30% stable, chronic, nonprogressive 32 patients 24 patients 24 patients Antiviral therapy 56 patients End-stage disease, HCC,liver transplantation, death Treatment failure (50%) Sustained response (50%) 28 patients 28 patients Projection of Lifetime Outcomesin HCV Infection Adapted from Alter HF, Seeff LB. Semin Liver Dis. 2000;20:17-35.
Factors Accelerating Progression of CHC Previous and concurrent alcohol consumption1 Older age at time of infection (>40 years)1 Male gender1 Other comorbidities: HIV/HCV coinfection2 HBV/HCV coinfection3 Obesity 1. Poynard T et al. Lancet. 1997;349:825-832. 2. Di Martino V et al. Hepatology. 2001;34:1193-1199.3. Lana R et al. Med Clin (Barc). 2001;117:607-610.
Utility of Diagnostic Tests Assessing Predicting Length Response Sustained Method Screen Confirmation of Therapy to Therapy Response ALT/AST X Enzyme Ximmunoassay (EIA) Supplemental assay X(RIBA*) HCV RNA qualitative X Xassay HCV RNA quantitative X Xassay HCV genotype X * No longer widely used CDC. MMWR. 1998;47(RR-19):1-39.
Role of Liver Biopsy in HCV Infection Assess severity of fibrosis and necroinflammation1,2 Confirm clinical diagnosis Evaluate possible concomitant disease processes (eg, alcoholic liver disease, NASH)1,2 Assess therapeutic intervention1 1. NIH Consensus Statement Online. Management of hepatitis C. 2. British Liver Trust Information Service. A guide to liver function tests.
Primary objective = cure No virus1 Arrest progression(necrosis/fibrosis) No symptoms Goals of Therapy Secondary objective = delay/prevent Reduce progression of fibrosis1 Reduce progression to cirrhosis2 Prevent decompensation Prevent HCC2 1. Worman HJ. Hepatitis C: current treatment. 2. Peters MG et al. Medscape HIV/AIDS eJournal. 2002;8(1). 3. Nishiguchi S et al. Lancet. 1995;346:1051-1055.
Who Should Be Treated ? Efficacy Normal ALT Mild Moderate Severe Cirrhosis Decompensated Tolerability / safety P R I O R I T Y
Virological Response:Definitions End-of-treatment response Undetectable HCV RNA levels at end of treatment (24 weeks for HCV genotype 2/3, 48 weeks for HCV genotype 1) Sustained virological response Undetectable HCV RNA levels at end of follow-up (24 weeks posttreatment) Nonresponse Detectable HCV RNA levels at the end of treatment Breakthrough Undetectable HCV RNA levels during treatment, but subsequently return to detectable HCV RNA levels Relapse HCV RNA negative at the end of treatment but subsequently positive during the follow-up period
Patterns of Virological Response Baseline Treatment Nonresponder Breakthrough HCV RNA Partialresponder Relapser Sustainedresponder (cure) Detection limit HCV RNA Undetectable 6 months Time
Optimizing IFN Alfa Pharmacokinetics Higher-dose IFN Optimized PK Serum Levels Conventional IFN Time 1 Week
Protein Pegylation Addition of polyethylene glycol (PEG) moiety to protein may result in1: Prolonged plasma half-life Reduced clearance Less immunogenicity Characteristics of new protein depend on1,2: Structure of PEG moiety (eg, size, branching, linkage bond strength) Site(s) of attachment to parent compound 1. Delgado C et al. Clin Rev Ther Drug Carrier Syst. 1992;9:249-304. 2. Hoffmann-La Roche. Roche Facets.
Mean Concentration-Time Profiles of Multiple-Dose Injections PEGASYS® 180 mg qw PEG-Intron™ 1200 Mon Tue Wed Thu Fri Sat Sun 0.5 mg/kg qw 1.0 mg/kg qw 1.5 mg/kg qw 30 1000 25 800 20 Concentration (pg/mL) 600 15 Concentration (ng/mL) 400 10 200 5 0 0 0 24 48 72 96 120 144 168 0 24 48 72 96 120 144 168 Hour Hour Modi MW. AASLD Annual Meeting. 2000. Adapted from Glue P et al. Clin Pharmacol Ther. 2000;68:556-567.
Pegylated IFNs:Dosing and Administration PEGASYS®2 PEG-Intron™1 WEIGHT-based dosing FIXED dose Lyophilized powder that needs to be reconstituted before each injection Dispensed as a stable solution ready for injection 1. PEG-Intron™. PDR®. 56th ed. 2002. 2. Perry CM, Jarvis B. Drugs. 2001;61:2263-2288.
Independent Host Factors Associated With SVR in Combination Therapy With PEGASYS® (Peginterferon Alfa-2a [40KD]) Factor Odds ratio P value HCV genotype (non-1 vs 1) 4.62 0.001 Baseline histology (F0/1/2 vs F3/4) 1.72 0.010 Baseline viral load ( 2 vs > 2 x 106 copies/mL) 1.47 0.004 0.001 Age ( 40 y vs >40 y) 1.39 Race 1.41 0.085 Body weight 0.99 0.949 Body surface area 0.86 0.484 Gender 0.82 0.160 Hoffmann-La Roche. Data on file. Updated from Hadziyannis SJ. EASL Annual Meeting. 2002.
Flu-like symptoms - Headache - Fatigue or asthenia - Myalgia, arthralgia - Fever, chills Nausea Anorexia Diarrhea Psychiatric symptoms - Depression - Insomnia Side Effects of IFN Treatment Alopecia Injection-site reaction Leukopenia Thyroiditis Autoimmunity Thrombocytopenia INTRON® A. PDR ®. 56th ed. 2002.ROFERON®-A. PDR ®. 56th ed. 2002.
Side Effects of RBV Treatment Hemolytic anemia Teratogenicity Cough and dyspnea Rash and pruritus Insomnia Anorexia REBETOL®. PDR®. 56th ed. 2002.Chutaputti A. J Gastro-enterol Hepatol. 2000;15(suppl): E156-E163.
Management of Patients Treated With IFN Plus RBV Monitoring and dose reduction for RBV-related anemia Monthly monitoring for pregnancy; emphasis on prevention Monitoring white blood cell and platelet counts Monitoring for evidence of depression REBETRON™. PDR ®. 56th ed. 2002.
Therapy of Chronic Hepatitis C Stopping Rule for HCV 1 PEG-IFN + Ribavirin week 12 PCR negative PCR positive > 2 log drop PCR positive < 2 log drop continue continue STOP week 24 PCR neg PCR pos continue STOP week 48 STOP STOP
Special At-Risk Patient Groups RBV-related risks - Significant cardiovascular disease - Hemoglobin level <12 g/dL in women, <13 g/dL in men - Noncompliance with contraception - Renal failure - Thalassemia IFN-related risk - Autoimmune diseases - Significant psychiatric disease
EPATITE VIRALE D • INCUBAZIONE: 30-180 gg(media 60-90) • TRASMISSIONE: parenterale,sessuale,salivare • CONTAGIOSITA’ come la forma B • EVOLUZIONE frequente verso la cirrosi,può evolvere in epatite fulminante mortale se associata a HBV
Viene trasmessa per via parenterale ( trasfusione sangue o emoderivati) o per via sessuale. I fattori di rischio sono simili a quelli della epatite B. Può esserci coinfezione con HBV oppure sovrainfezione nei soggetti portatori cronici, ma i soggetti immuni all’HBV da pregressa infezione o vaccinazione sono protetti dall’ HDV. L’infezione da virus D deve essere sospettata in caso di epatite B acuta particolarmente aggressiva o in caso di improvviso aggravamento in Paz portatore cronico. Nel caso di coinfezione si hanno fino al 20% di epatiti fulminanti (contro l’1 % della sola epatite B) mentre la sovrainfezione nei portatori cronici si ha cirrosi nel 90 % dei casi ’EPATITE B+D EVOLVE RAPIDAMENTE IN CIRROSI GRAVE
EPATITE VIRALE E • INCUBAZIONE: 14-60 gg(media 40) • TRASMISSIONE: parenterale,sessuale,salivare • CONTAGIOSITA’ come la A • EVOLUZIONE guarigione
Per il momento il virus della epatite E sembra essere localizzato in Asia ( Borneo, ex URSS, cine, Pakistan, India), Africa (Somalia), America Latina (Messico). Segnalati casi sporadici in Europa. E’ a trasmissione oro-fecale ed ha un andamento stagionale.