Download
1 / 25
260 likes | 671 Vues
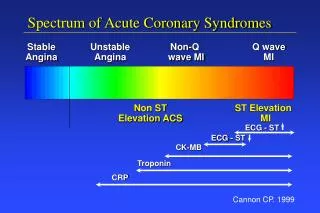
Unstable Angina /Non-ST Elevation Myocardial Infarction Critical Pathway Toolkit. Adapted from Dr Chris Cannon STRIVE Scientific Committee – 2008 Based on ACC/AHA Guidelines - 2007. Anticoagulants.

E N D
Unstable Angina /Non-ST Elevation Myocardial Infarction Critical Pathway Toolkit Adapted from Dr Chris Cannon STRIVE Scientific Committee – 2008 Based on ACC/AHA Guidelines - 2007
Anticoagulants • Enoxaparinmore effective in preventing combined end point of death or MI vsUnfractionated heparin (UFH). • Avoid cross-over during PCI Last SC dose >8 hrs, 0.3 mg/kg of iv. Last SC dose <8 hours, no additional enoxaparin.
Anticoagulants • Bivalirudin (single therapy) lower risk of bleeding compared to Enoxaparin and UFH. Approved only for early PCI. • Fondaparinux Lower risk of bleed but increased risk of catheter-related thrombi, to switch to UFH in Cath Lab.
Lipid Management • Fasting lipid profile workup within 24h [Class I, LOE: C] • Statin regardless of LDL-C [Class I, LOE: A]
Beta-blockers Ellis K, et al. 6-month mortality in ACS pts undergoing PCI 1.7% Beta-blockers vs 3.7% without beta-blockers. (Pooled results from EPIC, EPILOG, RAPPORT, CAPTURE and EPISTENT J Interv Cardiol 2003;16:299–305.)
Beta-blockers ACC/AHA 2007 Class 1 (LOE B)# Oral therapy initiated ≤24 h if NO • Heart failure • Low-output state • Increased risk for cardiogenic shock • Relative contraindications • PR ›0.24 s • 2nd or 3rd degree heart block • Reactive airway disease
Angiotensin-aldosterone inhibitors • Pulmonary congestion or LVEF ≤ 40% - ACEI within 24h or ARB if intolerant. • LV dysfunction, hypertension or diabetes – Long-term ACEI or ARB. • LVEF ≤ 40% and symptomatic heart failure or diabetes (without renal dysfunction/hyperkalemia) Aldosterone-receptor blockade in addition to ACEI.
Optimal Discharge Planning • Optimal blood pressure <140/90 mm Hg [Class I, LOE: A] <130/80 in diabetes or chronic kidney disease mm Hg [Class I, LOE: A] • Discharge education Medication use, cardiac rehabilitation, lifestyle modification (diet, exercise & smoking cessation) [Class I, LOE: C] • Follow-up 2-6 weeks in low risk, medically treated, revascularized, 14 days high risk [ Class I, LOE: C]