Download
1 / 24
261 likes | 1.6k Vues
Vogt-Koyanagi-Harada Syndrome. Laura S. Gilmore, MD Department of Ophthalmology November 12, 2004 Discussant: Leo Dominguez, MD. Case Presentation. CC : loss of vision and hearing

E N D
Vogt-Koyanagi-Harada Syndrome Laura S. Gilmore, MD Department of Ophthalmology November 12, 2004 Discussant: Leo Dominguez, MD
Case Presentation • CC: loss of vision and hearing • HPI: 38 yo HF with3 wk h/o progressively decreasing vision OD, irregular pupils. Seen by multiple MDs. Treated at onset for “allergies”, then by Ophtho in NM with PO prednisone at 80mg/day, PF and Atropine for about 1 week prior to presentation here. • PMH: No arthritis, RA, lupus, DM, HTN. +HepC. • POH: Poor vision OS since 10yo 2o trauma. No h/o glasses’ wear. • ROS: +Tinnitus, hearing loss, ocular pain, photophobia, scalp and hair tenderness, L occipital HA, poor balance/vertigo, hair/lash/brow thinning, hypopigmentation of face/arms, back pain.
Physical Exam • General: AAO, BP 110/61, pulse 53. Poor hearing, poor balance. • VA: 20/150 OD, LP OS • Pupils: 5 NR OU, irregularly shaped • External: Thin brows, lashes OU; splotchy white patches of skin over face, forehead, arms • SLE: KP OU; posterior synechiae OU; 4+C/F; 3+pigment on anterior capsule; 4+ vitreous cells • Lens: 2+NSC/2+PSC OU • B Scan: Serous RD OU; choroidal thickening; + vitreous cells
Differential Diagnosis • VKH • Posterior scleritis • Uveal effusion syndrome • Harada's disease • Acute posterior multifocal placoid pigment epitheliopathy • Sympathetic ophthalmia • Sarcoidosis
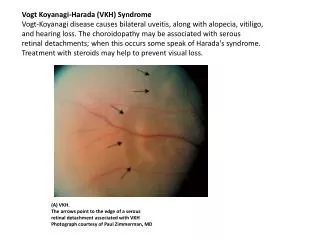
VKH • Uveoencephalitis • Extremely rare systemic disease of melanocyte-containing organs • Characterized by bilateral uveitis with associated cutaneous, neurologic, and auditory abnormalities • First described by Vogt in 1906 and Koyanagi in 1929 as anterior uveitis with poliosis, vitiligo, auditory disturbances (Vogt-Koyanagi syndrome) • Harada reported a pt in 1926 with idiopathic uveitis affecting posterior segment, RD, and meningeal irritation • Currently, VKH considered a single entity composed of variations of above symptoms
Etiology • Autoimmune response - Reaction against antigen (tyrosinase or tyr-related protein?) shared by uveal, dermal, and meningeal melanocytes - Circulating Ab against a retinal photoreceptor region - HLA-DR4 often present-commonly associated with other autoimmune diseases • Viral reactivation, possibly EBV • Immunogenic predisposition • Almost all cases are sporadic, with only rare familial cases • But, susceptibility associated with specific HLA groups, particularly DRB*0405
Demographics • Rare • No good data on frequency in US • Internationally, widely distributed • Darker pigmented pts • Range of presentation 10-52 years, maximum frequency in thirties • Women affected more
Clinical Presentation, Phase One • Prodromal (or meningeal) • Few days • HA, fever, photophobia, meningismus • Less common: gen muscle weakness, hemiparesis, dysarthria, aphasia • Altered mental status, from mild confusion to psychosis
Clinical Presentation, Phase Two • Uveitic • Several weeks • When pt’s typically seek medical attention, usually from Ophthalmologist • Bilateral blurred vision • Eye pain and irritation • Loss of vision • Tinnitus and dysacusis in 50%. May occur in any of the 3 phases of VKH
Clinical Presentation • Convalescent phase • Within 3 months of syndrome onset • Cutaneous signs • Usually after onset of uveitis • Have been reported years before any ocular sx • Patchy alopecia • Poliosis (in 90%) involving eyebrows, eyelashes, body hair and scalp • Symmetrical vitiligo (in 63%) over head and trunk
Diagnosis • American Uveitis Society guidelines • No ocular trauma or surgery • At least 3 of following 4: • B chronic inflammation of iris and CB • Posterior uveitis, including multifocal exudative RDs, and disc hyperemia or edema • Neurological signs of tinnitus, neck stiffness, CN or CNS dysfunction, cerebrospinal pleocytosis • Cutaneous findings of alopecia, poliosis, or vitiligo • A-scan and B-scan • Multidisciplinary management • Consider LP for CSF analysis, FA, audiometry, skin biopsy.
Treatment • Goal-reduce morbidity and prevent complications • Suppress initial intraocular inflammation • Early and aggressive systemic steroids • 60-100mg PO QD • Slow taper over 3-6 months • Unresponsive pts • Immunosuppression with azathioprine, cyclophosphamide, or methotrexate • Topical therapy • Steroid gtts • Cycloplegic-mydriatic gtts for sx relief
Prognosis • No mortality • Visual outcome depends on rapidity and appropriateness of tx • Uncommon to have long term complications • Reversible and irreversible vision loss • IOP elevation • Glaucoma • Cataracts • Hearing almost always completely resolves • Cutaneous pigmentary changes usually permanent
Back to Our Case • Hospital Admission 7/11/03 • IM, Rheumatology, Audiology, Gynecology • Labs: • daily CBC and BMP, ESR, toxoplasma, ACE, FTA-ABS, RPR, ANA, PPD, Lyme titer, lupus anticoagulant, anticardiolipin Ab, anti-dsDNA, SSA Ab, SSB Ab, HLA-B27, hepatitis panel, HIV, VDRL, antiproteinase III, UA, antimyeloperoxidase, beta-HCG, AP/lateral CXR and LXR, CT head/orbits, MRI head/orbits • Meds: • Solumedrol IV 1g/day per Rheum; PF gtt; atropine; pepcid; azathioprine 100mg/day; tacrolimus, 2.5mg PO BID
Results • MRI: • no inflammatory process in brain or surrounding structures • Labs: • ANA weakly positive, HepC +; all else normal or negative, X-rays nl • Audiology: • mild sensorineural hearing loss
Hospital Course • Improved hearing, balance, and visual acuity throughout hospital stay -VA 20/70 OD, LP OS -no cells/1+flare OU -decreased KP, vitreous cells -DFE: improved view OU; inferior SRD OD, almost 360o SRD OS • Discharged home at 1 week on PO Prednisone, Tacrolimus, Azathioprine, PF gtt, Atropine, Maxitrol ung
Relevant Clinical Course Since Discharge • 7/18/03-Discharged home, s/p 1 week IV steroid therapy, aggressive immunosuppression • 8/03-Timolol and Trusopt required for IOP 31, 34 • 10/17/03- 20/40 OD, CF @ 2ft OS, inflammation cleared, retina completely attached OU • 11/03-began tapering Prograff, Azathioprine (Rheumatology) • 12/03-began tapering PO prednisone and PF, d/c’d atropine
Clinical Course, Continued • 7/04-3-4+Uveitic PSC OU • 10/6/04-CE/PCIOL OD • 10/14/04-VA 20/30, very happy (with us) • Immunosuppression low-dose now • Currently on prednisone 20mg PO QD, azathioprine 50mg PO TID • Still requiring timolol and trusopt gtt
Conclusion • Very rare • Multidisciplinary treatment approach • Early and aggressive immunosuppression with slow, prolonged taper required to improve outcome and decrease long-term complications • Often have good outcomes
References • Choczaj-Kukula A, et al. Vogt-Koyanagi-Harada Syndrome: eMedicine.com. Sept 2003. • Fattal D. Vogt-Koyanagi-Harada Syndrome (VKH): summary and discussion of case presentation. Dept of Neurology, Baylor College of Medicine. 2001: www.bcm.tmc.edu/neuro1/index.html • Islam SM, et al. HLA class genes in VKH disease. Invest Ophthalmol Vis Sci. 1994. 35: 3890-3896. • Nussenblatt, RB, et al. Uveitis, Fundamentals and Clinical Practice. 1996. 312-324. • Snyder DA, et al. VKH syndrome. Am J Ophthalmol. 1980. 90: 69-75.