Download
1 / 39
390 likes | 519 Vues
The Evolving Role of LMWH in ACS. James J. Ferguson, MD Texas Heart Institute Houston, TX. Objectives. Assist peers in overcoming gaps in awareness of LMWH therapy in ACS Review emerging data for ACS NICE-3 GUSTO-IV Discuss strategies for increasing early administration of LMWH therapy

E N D
The Evolving Role of LMWH in ACS James J. Ferguson, MD Texas Heart Institute Houston, TX
Objectives • Assist peers in overcoming gaps in awareness of LMWH therapy in ACS • Review emerging data for ACS • NICE-3 • GUSTO-IV • Discuss strategies for increasing early administration of LMWH therapy • Discuss future directions for LMWH therapy in ACS
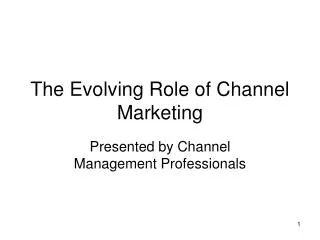
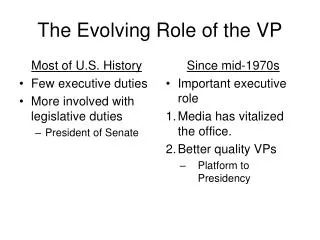
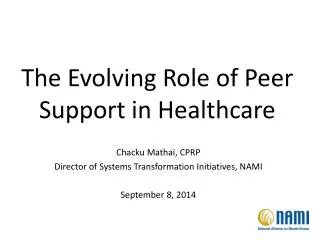
3910 B ESSENCE 8 3171 OVERALL 7081 5.3 4.1 0.77(0.62-0.96) 0.02 23 B 3910 B 14 ESSENCE 3171 B 0.79(0.65-0.96) 21 0.02 7081 6.5 5.2 OVERALL 3910 B 3171 43 ESSENCE B 0.82(0.69-0.98) 18 0.02 OVERALL 7081 8.6 7.1 TIMI 11B-ESSENCEMeta-Analysis Death/MI N Enox(%) Day UFH(%) % OR p TIMI 11B TIMI 11B TIMI 11B 0.5 0.6 0.7 0.8 0.9 1 2 Enox Better Odds Ratio UFH Better
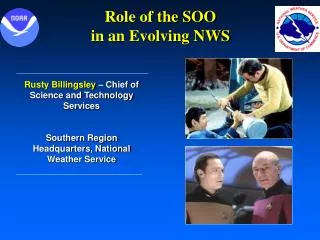
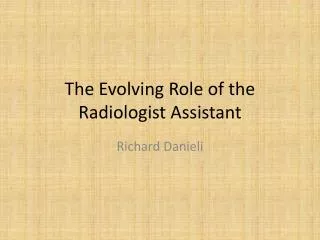
The ESSENCE Trial: 1-YearTime to First Triple Endpoint 40 35 30 25 20 Cumulative event rate (%) Heparin Enoxaparin 15 10 5 0 0 2 4 6 8 10 12 14 Months
Paradox • We have data strongly supporting a better form of therapy • We are still not using it widely Why?
AT IIa AT IIa AT Xa Xa AT Unfractionated Heparin LMW Heparin Upstream Downstream
Plasma Anti-Xa Activity after Ascending Single Doses of Subcutaneous Enoxaparin in Healthy Volunteers 2.0 1.8 1.0 mg/kg 1.25 mg/kg 1.6 1.5 mg/kg 2.0 mg/kg 1.4 1.2 Anti-Xa activity (IU/ml) 1.0 0.8 0.6 0.4 0.2 0.0 2 6 10 14 18 22 26 30 34 Time (h)
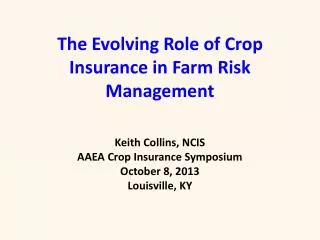
Death/MI/Urgent RevascEarly Rx Phase ESSENCE TIMI 11B 9 9 7.3 % 8 UFH UFH 8 ENOX ENOX 7 7 Aventis Parsippany, NJ 5.2 % 6 6 5 5.5 % 5 % Pts % Pts 4 4 RRR 24% P=0.03 4.2 % 3 3 RRR 18% P=0.21 2 2 1 1 0 0 72 8 16 24 32 40 56 64 0 0 8 16 24 32 40 48 56 64 72 48 Hours from Randomization Hours from Randomization Early Benefit
TIMI 11B Triple Endpoint at Day 43
Discussion • How are you currently using LMWHs? • What are you using? • When are you using it? • Why? Why not?
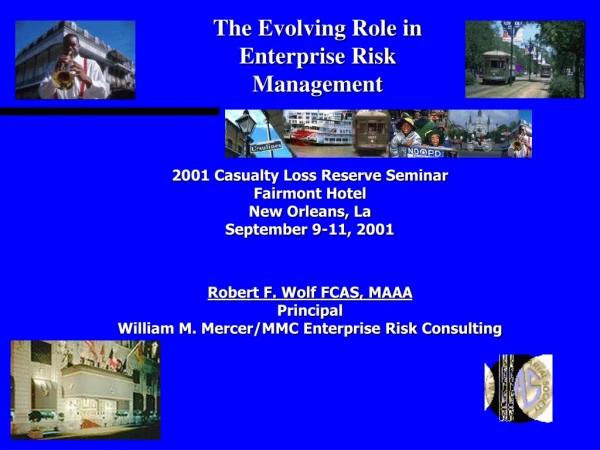
0.1 1 10 Better Worse Clinical Event Rates in Unstable Angina Trials † Preliminary results - placebo vs abciximab bolus plus 24 and 48 hr infusion ‡ Meta-analysis of TIMI 11B and ESSENCE at Day 43 Death / MI at 30 days Odds Ratio & 95% CI IIb/IIIa Placebo Trial (IIb/IIIa) N (%) (%) CAPTURE GUSTO IV† PRISM PRISM-Plus PURSUIT PARAGON Trial (LMWH) ESSENCE TIMI 11B TESSMA‡ 1252 7800 3231 1570 10,948 2282 3171 3910 7,081 4.8 ~8.6 5.7 8.7 14.2 10.3 Enoxaparin 6.2 7.4 7.1 9.0 8.0 7.0 11.9 15.7 11.7 Heparin 7.7 8.3 8.6 N
NICE-3National Investigators Collaborating on Enoxaparin XXIInd Congress of the European Society of Cardiology August 30, 2000 Amsterdam, The Netherlands
NICE-3 Objectives • To assess the safety profile (primarily with respect to bleeding) of enoxaparin and a IIb/IIIa antagonist (abciximab, eptifibatide or tirofiban) in patients with ACS • To assess the feasibility and safety of bringing patients to the cath laboratory on combination therapy (without the use of UFH)
NICE-3Inclusion Criteria • Recent (w/in 24 hours) unprovoked or rest angina • Documented ischemic CAD • ECG changes • Abnormal biomarkers • Previously documented CAD • Patients on prior UFH could be included
NICE-3Exclusion Criteria • Evolving Q-wave MI • Fibrinolytic Rx w/in 48 hours • Cardiogenic shock • Left main disease • Valvular disease • CABG w/in 2 mos.; revasc w/in 1 week • Thrombocytopenia
All treated with Enoxaparin Eptifibatide (n=252) Abciximab (n=147) Tirofiban (n=217) NICE-3Protocol 661 patients enrolled 46 clinical sites in US/Canada Study Initiated January 2000 [Enoxaparin alone] (n=45) Enrollment Completed May 2000 If patients went to the cath lab, combination Rx continued; no UF heparin used If within 8 hrs of last enoxaparin, no additional Rx If > 8 hrs from last dose, 0.3 mg/kg enoxaparin iv All IIb/IIIa patients (n=616) In-hospital, 14-day, and 30-day follow-up Data available August 2000
NICE-3Protocol • Primary Endpoint • Non-CABG major bleeding (TIMI criteria) during hospitalization • Secondary Endpoints • Minor bleeding (TIMI criteria) • Clinical efficacy • Composite of death, MI, ischemia-driven TVR
NICE-3Sample Size • Primary Hypothesis • The 95% CI for major bleeding will not exceed the historical rate • Agents examined as a whole and separately • Example (Assuming major bleed rate of 2%): • A 200 patient sample size has a 95% CI of approx 0.1-3.9% • A 150 patient sample size has a 95% CI of approx0-4.2%
NICE-3Demographics • Age 62.9 12.2 years • Weight 83.9 18.5 kg • M/F approx 2:1 • LOS 5.9 4.2 days • History • HTN 63.5% Prior PCI 30.7% • DM 30.0% Prior CABG 20.9% • Smoking 28.1% Prior MI 36.2% • CHF (on admin) 4.5%
NICE-3Bleeding (%) Enoxaparin All IIb/IIIa (n=616) [Enoxaparin alone] (n=45) Tirofiban (n=217) Eptifibatide (n=252) Abciximab (n=147) All 27.9 Major 4.5 non-CABG 1.9 Minor 25.0 Xfusion 10.5 All 17.8 Major 6.7 non-CABG 4.4 Minor 13.3 Xfusion 8.9 All 27.2 Major 5.1 non-CABG 1.4 Minor 24.0 Xfusion 10.6 All 30.6 Major 4.4 non-CABG 3.2 Minor 27.2 Xfusion 10.3 All 24.5 Major 4.1 non-CABG 0.7 Minor 22.4 Xfusion 10.9
NICE-3In-Hospital Clinical Outcomes (%) Enoxaparin All IIb/IIIa (n=616) [Enoxaparin alone] (n=45) Tirofiban (n=217) Eptifibatide (n=252) Abciximab (n=147) Death 0.3 MI 3.4 uTVR 2.1 D/MI/uTVR 5.7 D/MI 3.6 Death 0 MI 2.2 uTVR 2.2 D/MI/uTVR 4.4 D/MI 2.2 Death 0.5 MI 4.1 uTVR 3.2 D/MI/uTVR 7.8 D/MI 4.6 Death 0.4 MI 3.2 uTVR 2.0 D/MI/uTVR 5.2 D/MI 3.2 Death 0 MI 2.7 uTVR 0.7 D/MI/uTVR 3.4 D/MI 2.7
NICE-330% in Platelet Count 1.44%<100K 0<100K 0.85%<100K 0.86%<100K (n=138) (n=235) (n=208) (n=581) (n=38)
NICE-3All Major Bleeding (%) 6 Abciximab Eptifibatide Tirofiban All IIb/IIIa 4.8 4.8 4 4.3 3.6 3.1 2 1.7 1 0.9 0 Patients not undergoing PCI or CABG Patients undergoing PCI
NICE-3PCI Patients (n=292) Non-CABG Major Bleeding Tirofiban 0.9% Eptifibatide 2.4% Abciximab 0 All IIb/IIIa 1.0%
NICE-3Conclusions • Combination of enoxaparin and IIb/IIIa • Does not result in excess major bleeding • Events (non-CABG) • Patients on combination Rx can safely undergo PCI • Clinical outcomes in NICE-3 were comparable to those noted in prior studies • Therefore, not necessary to use UFH in: • UA/NSTEMI patients undergoing coronary • intervention who are treated with enoxaparin and an IV IIb/IIIa antagonist
NICE-3Clinical Implications • Real-world study • Broad distribution of patients and institutions • Safety data for all 3 commercially available • IIb/IIIa antagonists • Addresses safety concerns about combining enoxaparin and a IIb/IIIa antagonist • Addresses logistical concerns about transition to cath lab • Foundation for future investigations
Issues for Enoxaparin in ACS No safety issues at present Potential synergism Good regimen for PCI Is it safe to combine enoxaparin with IIb/IIIa blockers? How do we make the transition from the floor to the cath lab? Carefully but confidently, within the limits of our experience
Discussion • How does NICE-3 help you? • What questions doesn’t it answer? • Is it going to affect your practice? • What additional information do we need?
The NICE Trials Together PI: Cindy Grines Enoxaparin (1 mg/kg iv) for PCI PI: James Ferguson Enoxaparin (1 mg/kg sq) with IIb/IIIa blocker for ACS (including PCI) NICE-1 NICE-3 NICE-4 ? ? ? PI: Dean Kereiakes Enoxaparin (0.75 mg/kg iv) with abciximab for PCI
Discussion Patient management strategies when an ACS patient, who is a candidate for LMWH, proceeds to the cath lab
Future Data GUSTO-IV ACS A to Z ACUTE-2 INTERACT CRUISE [Pilot trial LMWH vs combo Rx] [Efficacy trial LMWH vs UFH]
GUSTO-IV ACSSimoons, ESC 2000 • Multicenter study (458 sites in 24 countries) • ACS patients not undergoing revascularization • Treated with ASA and UFH • Scandanavian subset got LMWH • 7800 patients randomized to • abciximab (24 hours) • abciximab (48 hours) • placebo • Primary Endpoint: Death or MI at 30 days
GUSTO-IV ACSSimoons, ESC 2000 • Definition of ACS: Rest angina with ST-segment (1/2 mm) or (+) troponin • Coronary angiography only for recurrent ischemia • ~ 28% had evolving MI • 14% from US, 48% from Western Europe • ~80% had ST-segment • ~59% had + troponin • ~32% had both • Revasc performed in ~30% by day 30 • Only 1.4% revasc in first 48 hours
GUSTO-IV ACS 48 Hours 7 Days 30 Days
GUSTO-IV ACS LMWH Substudy ICH Ischemic Stroke