
Ureterocele
Ureterocele. Saccular out-pouching of the distal ureter into the urinary bladder Arise from abnormal embryogenesis, with anomalous development of the intravesical ureter, the kidney, and the collecting system

Ureterocele
E N D
Presentation Transcript
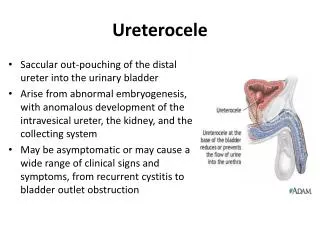
Ureterocele • Saccular out-pouching of the distal ureter into the urinary bladder • Arise from abnormal embryogenesis, with anomalous development of the intravesical ureter, the kidney, and the collecting system • May be asymptomatic or may cause a wide range of clinical signs and symptoms, from recurrent cystitis to bladder outlet obstruction
Types of ureteroceles classified by their association with the renal unit • Single-system ureteroceles • associated with a single kidney, a single collecting system, and a solitary ureter • Duplex-system ureteroceles • associated with kidneys that have a completely duplicated collecting system and 2 ureters. • Orthotopicureterocele • orifice is located in a normal anatomic (orthotopic) position within the bladder • usually arises from a single renal unit with one collecting system and is more common in adults • Ectopic ureterocele • orifices are located in an ectopic position, such as the bladder neck or urethra • arise from the upper pole moiety of a duplicated collecting system and are more common in the pediatric population
Classification based on the features of the affected ureteral orifice • Stenoticureteroceles • located inside the bladder with an obstructing orifice • Sphinctericureterocele • refers to those that lie distal to the internal sphincter • the ureterocele orifice may be normal or patulous, but the distal ureter leading to it becomes obstructed by the activity of the internal sphincter • Sphincterostenoticureteroceles • have characteristics of both stenotic and sphinctericureteroceles • Cecoureteroceles • elongated beyond the ureterocele orifice by tunneling under the trigone and the urethra
Etiology • Several theories exist, including: • obstruction of the ureteral orifice • incomplete muscularization of the intramural ureter • excessive dilatation of the intramural ureter during the development of the bladder and trigone • Obstruction of the ureteral orifice during embryogenesis, with incomplete dissolution of the Chwalla membrane • the most commonly accepted theory behind ureterocele formation • Chwalla membrane • primitive thin membrane that separates the ureteral bud from the developing urogenital sinus • failure to completely perforate during development of the ureteral orifice is thought to explain the occurrence of a ureterocele
Epidemiology • 1 in every 4000 children • Most commonly in white persons • F:M ratio - 4-7:1 • Although a slight left-sided preponderance appears to exist, approximately 10% of ureteroceles occur bilaterally • Ectopic ureteroceles has been reported to be approximately 80% in most pediatric series • Similarly, approximately 80% of ureteroceles are associated with the upper pole moiety of a duplex system • Single-system ectopic ureteroceles are uncommon and are most often found in males
Pathophysiology Embryogenesis of the kidney and ureter • Ureteral bud: primitive analog of the ureter, branches off the caudal portion of the Wolffian (mesonephric) duct during the first 4-6 weeks of gestation • Cranial portion of the ureteral bud: joins with the metanephricblastema, a primitive analog of the kidney, and begins to induce nephron formation • The ureteral bud subsequently branches into the renal pelvis and the calyces and induces nephron formation • Caudally, the mesonephric duct and the ureteral bud are incorporated into the cloaca (urogenital sinus) as it forms the bladder trigone • At this point, the Chwalla membrane perforates to allow the formation of a normal ureteral orifice • If the membrane does not completely perforate, an orthotopicureteroceleresults
Because the lower pole ureteral bud is absorbed more rapidly, the detrusorsubmucosal tunnel becomes short • This short submucosal tunnel predisposes the lower pole ureter to reflux • In contrast, the upper pole ureteral bud is absorbed slowly, resulting in a long submucosal tunnel • At this point, the Chwalla membrane must perforate to allow the formation of a normal ureteral orifice • This results in an ectopic ureter • If the Chwalla membrane does not perforate completely, a ureterocele results, most likely in an ectopic location
Clinical Manifestations • Urinary tract infection • Urosepsis • Obstructive voiding symptoms • Urinary retention • Failure to thrive • Hematuria • Cyclic abdominal pain • Ureteral calculus
Diagnostic Procedures • Laboratory Studies • Urinalysis • Urine culture • Complete blood cell count • Serum chemistries, especially BUN and serum creatinine • Blood cultures • Fungal cultures: obtained in infants who have been on long-term antibiotic therapy or in immunocompromised patients with clinical evidence of UTI
Imaging Studies • Renal or bladder ultrasonography • First-line imaging study for evaluating the upper and lower urinary tract in the pediatric population • Seen as a fluid-filled cystic intravesical mass • Aka "cyst within a cyst" • Hydroureteronephrosis is noted as a dilatation of renal pelvis and the proximal ureter • Also provides information on the thickness of renal cortex and echogenicity of renal parenchyma • Degree of echogenicity is indirectly proportional to the degree of renal dysplasia that is present • Bladder ultrasonography documents the efficiency of bladder emptying by noting the amount of postvoid residual urine that is present
Voiding cystourethrography • Appears as a smooth, round filling defect along the base of the bladder • Can be used to document the efficiency of bladder emptying with assessment of the amount of postvoid residual urine that is present • Vesicoureteral reflux of the ipsilateral lower pole ureters approaches 50%, whereas only 25% of the contralateral renal units have vesicoureteral reflux • Vesicoureteral reflux into the ureterocele is rare, but it may occur following spontaneous ureterocele rupture or after unroofing of the ureterocele
Diuretic nuclear renography (nuclear renal scan) • Nuclear renal scan using technetium 99m diethylenetriaminepentaacetic acid (DTPA) is an excellent study for establishing the differential renal function objectively and the efficiency of drainage of the dilated collecting system (washout times) • DTPA is cleared almost exclusively by glomerular filtration • Its rate of clearance provides an excellent estimate of glomerular filtration rate (GFR) • Alternatively, technetium 99m mercaptoacetyltriglycine (MAG3) may be used • This radioisotope is rapidly cleared by tubular secretion and is not retained by the kidneys • MAG3 is an excellent replacement for DTPA (eg, diuretic renography) in the pediatric population
Intravenous pyelography • Useful for delineating renal anatomy and providing a subjective estimation of relative renal function • The following may be seen on IVP: • Hydronephrosis, revealing dilatation of collecting system • Hydronephrotic upper pole displacing the lower pole moiety laterally and inferiorly (ie, the "drooping lily") • Ureteral displacement by the hydroureter or hydronephrotic upper pole moiety • Cobra-head extension of the distal ureter (ureterocele) (seen in adults)
Magnetic resonance imaging • Excellent anatomical study for evaluating rare cases with suspected dysplastic, nonfunctioning, ectopic renal moieties and ectopic ureteral insertion
CT scanning of the abdomen and pelvis • If renal ultrasonography and IVP findings are equivocal, CT scanning may provide additional clues for diagnosing simple or ectopic ureterocele • Can reveal the presence of a duplicated collecting system, hydronephrotic upper pole segment, or dysplastic upper pole moiety
Cystoscopy, vaginoscopy, or retrograde pyelography • Endoscopic procedures that allow direct inspection and examination of the lower urinary tract, as well as the female genitalia • For optimal demonstration of a ureterocele, one must examine the bladder when it is both full and empty • When radiologic suspicion of a ureterocele in an adult is aroused, cystoscopy often confirms radiographic findings • If clinically indicated, the ureterocele may be treated with endoscopic incision or unroofing at the same setting
Treatment • Medical Therapy • Observation alone is rarely a good option in symptomatic ureteroceles • Must rapidly initiate aggressive antibiotic therapy • Antibiotics should be instituted during the initial diagnostic evaluation and during surgical intervention
Surgical Therapy Goals of treatment include the following: • Control of UTI • Preservation of renal function • Protection of ipsilateral and contralateral renal units • Maintenance of urinary continence
Surgical Therapy Surgical approach is selected based on the following: • Age of the patient • Size and location of ureterocele • Degree of renal function • Presence and degree of vesicoureteral reflux • Comorbid conditions (risk of anesthesia)
Endoscopic incision • Least invasive method for decompressing the ureterocele • Ideal method for dealing with a neonate with ureterocele-induced obstructive uropathy and sepsis • Performed via the cystoscope, a small puncture is created at the base of the ureterocele • In addition to its therapeutic value, this technique may be used when the contribution of the associated renal moiety to overall renal function is indeterminate • Also allows palliative decompression in children at high risk (secondary to concurrent medical illness), so that definitive reconstruction can be delayed until an adequate healing period has occurred • Definitive therapy in only 10-40% of patients with ectopic ureteroceles, compared to 90% of the patients with a single system intravesicalureterocele
Upper pole heminephrectomy and partial ureterectomy • Involves removal of the upper pole of the kidney, as well as the affected proximal ureter to the level of iliac vessels • Remaining distal ureterocele is not excised but rather is decompressed • Definitive treatment in patients with an obstructed ectopic ureterocele and a dysplastic upper pole, but without associated vesicoureteral reflux • Excellent first-line procedure for the child with a ureterocele that affects only the ipsilateral upper pole • Good choice in the child with a ureterocele with only ipsilateral renal involvement (which may include upper pole obstruction and lower pole reflux, for example)
Ureteropyelostomy • Operation that joins the upper pole ureter to the lower pole renal pelvis • Preferred if the affected renal unit demonstrates significant function • Alternatively, a high ureteroureterostomy may also be performed • This is true for both pediatric and adult populations
Excision of the ureterocele and ureteralreimplantation • Indicated as a primary procedure if the patient has significant vesicoureteral reflux in the lower pole moiety and a well-functioning upper pole moiety and/or significant contralateralvesicoureteral reflux • Both ipsilateralureters may be reimplanted within a common sheath or via ureteroureterostomy • This operation is commonly delayed until the child is older (aged approximately 2 y/o) • However, this operation should be performed before the child is toilet trained since it is rather extensive surgery
In the pediatric population, the excision and reimplantation procedure commonly is used as a secondary procedure (after previous heminephrectomy or endoscopic incision of a ureterocele) because of UTI, voiding disturbance, persistent vesicoureteral reflux, or obstruction • If this procedure is selected as the first-line treatment in the appropriate patient, the rate of secondary surgery is low
Nephroureterectomy • Performed in patients with single system ureterocele and a nonfunctioning kidney • The traditional method of correcting an ectopic ureterocele in a duplex system has been to perform a total reconstruction • This involved a bladder surgery, followed by renal surgery • The bladder surgery required excision of a ureterocele, reconstruction of the detrusor, and reimplantation of the ipsilateralureter. • This was followed by a flank incision and upper pole heminephrectomy • Since most ureteroceles typically present in young children (often <1 y), total reconstruction was technically challenging, and complications were common
Complications • Endoscopic incision of ureterocele • Iatrogenic VUR occurs in 40-50% of pediatric patients • This is infrequently definitive therapy, except in cases of a single system intravesicalureterocele • Upper pole heminephrectomy • Highest risk of intraoperative blood loss • Vascular compromise of lower pole with potential loss of renal function • Need for further lower tract reconstruction due to persistent reflux, infection, or failure to decompress the ureterocele • Excision of ureterocele and ureteralreimplantation • Problematic hematuria and/or bladder spasms • Damage to bladder neck or continence mechanism • Injury to the contralateralureteral orifice • Compromise of blood supply to the lower pole ureter