Download
1 / 32
480 likes | 1.18k Vues
Mechanism of Drug Action Dr. Syed Ayaz Ali M.Pharm; Ph.D Associate Professor & Head Dept. of Pharmacology Y.B.Chavan College of Pharmacy Aurangabad. Mechanism of Drug Action. Pharmacodynamics

E N D
Mechanism of Drug Action Dr. Syed Ayaz AliM.Pharm; Ph.DAssociate Professor & HeadDept. of PharmacologyY.B.Chavan College of PharmacyAurangabad
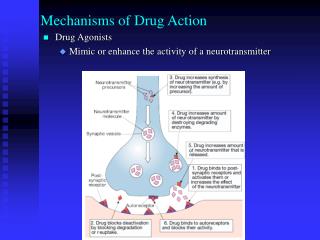
Mechanism of Drug Action Pharmacodynamics • Pharmacodynamics is concerned with the actions, interactions and the mechanism(mode) of action of drugs. • Some drug-receptor interaction are highly specific • (Pharmacological receptors are involved) & • some are non-specific (receptors are not involved). DRUGS Pharmacological receptors Without receptors
Molecular & Biochemical Mechanism of Drug Action The protein targets for drug action on mammalian cells can be broadly divided into: Receptors Ion channels Enzymes Carrier molecules (transporters)
Receptors • They are protein structure present on the mammalian cell or within the cells. • Receptors are the sensing elements in the system of chemical communications that coordinates the function of all the different cells in the body. • The chemical messengers being the various • Hormones • Neurotransmitters • other mediators (e.g. Autocoids: Histamine, 5HT, etc) • Many therapeutically useful drugs act, either as agonists or antagonists, on receptors for known endogenous mediators.
Drugs which act via receptors: Act at low concentrations Show SAR Can be antagonized by specific antagonists Examples: Acetylcholine, Adrenaline, Histamine etc.
Ion Channels Some ion channels (known as ligand-gated ion channels or ionotropic receptors) incorporate a receptor and open only when the receptor is occupied by an agonist; others are gated by different mechanisms, e.g. voltage-gated ion channels are particularly important. In general, drugs can affect ion channel function by interacting either with the receptor site of ligand-gated channels, or with other parts of the channel molecule. The interaction can be indirect, involving a G-protein and other intermediaries, or direct, where the drug itself binds to the channel protein and alters its function.
Example : Voltage gated-sodium channels are blocked by local anesthetics.Examples of drugs that bind to accessory sites on the channel protein and thereby affect channel gating include: Dihydropyridine, vasodilator drugs, which inhibit the opening of L-type calcium channels.benzodiazepine tranquillizers, these drugs bind to a region of the GABA receptor-chloride channel complex .Sulfonylureas (Antidiabetics), which act on ATP-sensitive potassium channels of pancreatic β-cells and thereby enhance insulin secretion.
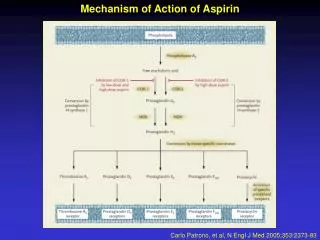
Enzymes Many drugs are targeted on enzymes. Here the drug molecule is a substrate analogue that acts as a competitive inhibitor of the enzyme either reversibly (e.g. Neostigmine, acting on acetylcholinestrase) or the binding is irreversible and non-competitive (e.g. Aspirin, acting on cyclo-oxygenase). Drugs may also act as false substrates, where the drug molecule undergoes chemical transformation to form an abnormal product that subverts the normal metabolic pathway. Example is the anticancer drug fluorouracil
Carrier molecules (transporters) The transport of ions and small organic molecules across cell membranes generally requires a carrier protein, because the permeating molecules are often too polar (i.e. insufficiently lipid-soluble) to penetrate lipid membranes on their own. There are many examples of such carriers : Glucose and amino acid transporter, Ion & organic molecule transporters, neurotransmitter precursors (such as choline) or of neurotransmitters (Noradrenaline, 5-HT, glutamate uptake).
The amine transporters belong to a well-defined structural family, distinct from the corresponding receptors.The carrier proteins embody a recognition site that makes them specific for a particular permeating species.These recognition sites can also be targets for drugs whose effect is to block the transport system. e.g. TCA, Cocaine, Omeprazole, Cardiac Glycosides
TYPES OF RECEPTORReceptors elicit many different types of cellular effect.Based on molecular structure and the nature of transduction mechanism four receptor types can be distinguished. Effects • Synaptic transmission • Catecholamines • Thyroid & Steroid Hormones • Peptides Operating Time • Milliseconds • Seconds • Hours or days • Longer time
Type 1: Ligand-gated ion channels (ionotropic receptors). These are membrane proteins with a similar structure to other ion channels, and incorporate a ligand-binding (receptor) site, usually in the extracellular domain. On these receptors fast neurotransmitters act. Examples include the nicotinic acetylcholine receptor; GABAA receptor; glutamate receptors of the NMDA.
These ion channels have same structural features e.g. Nicotinic Ach Receptor It is assembled from 4 different types of subunit αβγδ. These subunits are inserted into the membrane. The oligomeric structure possesses two Ach binding sites, each lying at the interface between one of the 2 subunits and its neighbor. Both must bind Ach molecules in order for the receptor to be activated.
Type 2: G-protein-coupled receptors (GPCRs). metabotropic receptors They are membrane receptors that are coupled to intracellular effector systems via a G-protein . They constitute the largest family, and include receptors for many hormones and slow transmitters. Example the muscarinic acetylcholine receptor, Adrenoceptors & Chemokine receptors. Subtypes are also present and all have same basic structure.
Type 3: Kinase-linked and related receptors. This is a large and heterogeneous group of membrane receptors responding mainly to protein mediators. They comprise an extracellular ligand-binding domain linked to an intracellular domain by a single transmembrane helix. In many cases, the intracellular domain is enzymic in nature (with protein kinase or guanylyl cyclase activity). Examples: Type 3 receptors includes for those insulin and for various cytokines and growth factors.
Type 4: Nuclear receptors. These are receptors that regulate gene transcription. The term nuclear receptors is something of a misnomer, because some are actually located in the cytosol and migrate to the nuclear compartment when a ligand is present. They include receptors for steroid hormones, thyroid hormone, and other agents such as retinoic acid and vitamin D.
Receptor Concept The concept of drugs acting on receptors generally is credited to John Langley (1878). While studying the antagonistic effects of atropine against pilocarpine -induced salivation. The word receptor was introduced in 1909 by Paul Ehrlich. Ehrlich postulated that a drug could have a therapeutic effect only if it has the "right sort of affinity." Ehrlich defined a receptor in functional terms: ". that combining group of the protoplasmic molecule to which the introduced group is anchored will hereafter be termed receptor.“ The receptors are specialized target macromolecules present on the cell surface or intracellularly. Receptors bind drugs & initiate events leading to alterations in biochemical and/or biophysical activity of a cell and consequently, the function of an organ. Drug Receptors From a numerical standpoint, proteins form the most important class of drug receptors. Examples include the receptors for hormones, growth factors, transcription factors, neurotransmitters; the enzymes (e.g., dihydrofolate reductase, acetylcholinesterase, and cyclic nucleotide phosphodiesterases)
Drug-Receptor Interaction The binding of drugs to receptors can involve all known types of interactions-ionic, hydrogen bonding, hydrophobic, vander Waals, and covalent. Most interactions between drugs and their receptors involve bonds of multiple types. If binding is covalent, the duration of drug action is frequently, but not necessarily, prolonged. Noncovalent interactions of high affinity also may be essentially irreversible. The magnitude of the responses is proportional to the number of drug-receptor complexes. Drug + K1 Drug-receptor complex K3 (Response) Receptor K2 WhereK1, K2 and K3 are rate constants. The rate at which the drug molecule combines with a receptor site is K1. Similarly, the rate at which the drug-receptor complex dissociates is given by K2. The rate at which a response is generated following a drug-receptor interaction is given by rate constant K3. These constants are used to define some basic concepts related to drug-receptor interactions.
In general, the drug-receptor interaction is characterized first by binding of drug to receptor and second by generation of a response in a biological system. The first function is governed by the chemical property of affinity, ruled by the chemical forces that cause the drug to associate reversibly with the receptor. AffinityIt describes the ability of a drug to form and subsequently maintain a complex with a receptor site.Intrinsic ActivityIt describes the ability of a drug to evoke a pharmacologic response on combining with a receptor. E.g. Acetylcholine acts as a cholinergic agonist.
Potency & EfficacyPotency: A drug is said to be potent when it possesses high intrinsic activity at low unit weight doses. Knowledge of a drug’s potency is important for finding out the appropriate dosage level to be administered .Efficacy: It refers to the maximal or peak response produced by a drug, and is an important determinant in the drug selection process.Intensity of Drug ResponseThe magnitude of the response elicited by a drug-receptor interaction can vary widely. Currently three theories attempt to explain the nature of drug-receptor interactions and their relationship to the response produced:1) The receptor occupation theory2) The rate theory3) Theories involving drug-induced protein changes at receptor site.The receptor occupation theory :This theory postulates that the magnitude of the response produced by a drug is directly proportional to the number of receptors occupied. A maximal drug effect occurs when all the receptors are occupied.
The Rate Theory:This theory postulates that the intrinsic activity of the drug is related to the rate of complex formation (k1), and the rate of complex breakdown (k2), which are in turn the measures of association and dissociation of the drug with the receptor.The agonist have high rate of association and dissociation, and it is this turnover number which decides the magnitude of the response. In contrast, the antagonists produce a stable complex with the receptor that does not readily breakdown, thereby preventing the interaction of the agonist with the receptor. Theories involving drug-induced protein changes at receptor site:Certain theories suggest that the agonist exerts its action by inducing some temporary structural changes in the protein constituents at the receptor site. Such structural alterations modify the permeability of cell membranes and produce a response. Possibly antagonists produce structural changes that prevent the formation of an agonist-receptor complex.Importance of the receptor conceptIt is important that we understand the roles and functions of receptors because most drugs interact with receptors that will determine selective therapeutic and toxic effects of the drugs. Moreover, receptors largely determine the quantitative relations between dose of a drug and pharmacologic effect.
Some important terms related to drugs and receptors:Agonist: It is a drug (or hormone or neurotransmitter) which combines with its specific receptor, activates it and initiate a response e.g. acetylcholine, noradrenalineactivate cholinoceptors and adrenoceptors respectively.Antagonist: It is a drug which binds to the receptor, but does not activate it. Moreover, it prevents the action of the agonist by rendering the receptor unavailable for interaction with the agonist e.g. atropine antagonizes acetylcholine. A pure antagonist has no action of its own, but acts only by interfering with the action of an agonist e.g. the opioid antagonist naloxone.Partial Agonist: It is a drug that binds to the receptor, but activates it weakly and prevent the action of a full agonist. This drug acts on the receptor with an intrinsic activity or efficacy of less than one.A unique feature of these drugs is that, under appropriate conditions, a partial agonist may act as an antagonist of a full agonist. e.g. Aripiprazole, an atypical neuroleptic agent, is a partial agonist at selected dopamine receptors. Dopaminergic pathways that were overactive would tend to be inhibited by the partial agonist, whereas pathways that were underactive may be stimulated.
Inverse Agonist: It is a drug that causes an effect opposite to that of the agonist, in contrast to a competitive antagonist that simply blocks the agonist, but has no inherent action of its own.E.g. The agonist action of benzodiazepines on the GABA receptor produces sedation, anxiolysis, muscle relaxation and controls convulsions.The inverse agonist: The β-carbolines (e.g. n-butyl-β-carboline-3-carboxylate) also binds to GABA receptor causing stimulation, anxiety, increased muscle tone and convulsions.Mixed Agonist-Antagonist: It is a drug that acts simultaneously on a mixed group of receptors with an agonist action on one set, and with an antagonist action on another set.e.g. opioids. Some mixed agonist-antagonist drugs, such as pentazocine and nalorphine, can produce severe psychotomimetic effects that are not reversible with naloxone (suggesting that these undesirable side effects are not mediated through classical opioid receptors). Also, pentazocine and nalorphine can precipitate withdrawal in opioid-tolerant patients. For these reasons, the clinical use of these mixed agonist-antagonist drugs is limited.
Signal Transduction by GPCRsGPCRs control many different aspects of cell function by acting on a variety of different signal transduction mechanisms.The link between the membrane receptor and the first stage of the signal transduction cascade is established through the G-proteins.G-Proteins and their roleG-proteins represent the level of middle management in the organizational hierarchy, intervening between the receptors and the effector enzymes or ion channels.They are called as G-proteins because of their interaction with the guanine nucleotides GTP and GDP. GPCRs are sometimes called as metabotropic receptors.All are monomers comprising seven membrane-spanning segments .One of the intracellular loops is larger than the others and interact with the G-protein.The G-protein is a membrane protein comprising three subunits (alpha, beta, gamma), the alpha-subunit possessing GTPase activity.There are three main classes of G-proteins (Gs, Gi, Gq).
Gs and Gi produce, respectively , stimulation and inhibition of the enzyme adenylate cyclase and a similar bidirectional control operates on other effectors, such as phospholipase C.
TARGETS FOR G-PROTEINS • The main targets for G-protein through which GPCRs control different aspects of cell function are: • Adenylate Cyclase : the enzyme responsible for cAMP formation. • Phospholipase C: the enzyme responsible for inositol phosphate and diacyglycerol formation. • Ion channels: particularly calcium and potassium channels. The Adenylate Cyclase / cAMP system • cAMP is a nucleotide synthesized within the cell from ATP by the action of a membrane bound enzyme adenylate cyclase. • cAMP is produced continuously and inactivated by hydrolysis to 5’-AMP through the action of phosphodiesterases.
Many different drug, hormones and neurotransmitters act on GPCRs and produce their effects by increasing or decreasing the catalytic activity of adenylate cyclase, thus raising or lowering the concentration of cAMP within the cell.