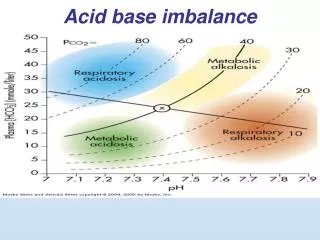
Acid base imbalance
Acid base imbalance. Rafat Mosalli MD FAAP FRCPC. Objectives. Define the terms acidosis and alkalosis. How to do blood gas interpretation

Acid base imbalance
E N D
Presentation Transcript
Acid base imbalance Rafat Mosalli MD FAAP FRCPC
Objectives Define the terms acidosis and alkalosis. How to do blood gas interpretation Explain how the acid-base balance of the blood is affected by C02 and HC03-, and describe the roles of the lungs and kidneys in maintaining acid-base balance.
Acid-Base Balance It is the regulation of HYDROGEN ions. (The more Hydrogen ions, the more acidic the solution and the LOWER the pH) The acidity or alkalinity of a solution is measured as pH
HH equation pH = 6.1 + log [HCO3-] 0.03 x Pco2
Normal Arterial Blood Gas Values* pH 7.35 - 7.45 PaCO235 - 45 mm Hg PaO2 70 - 100 mm Hg ** SaO2 93 - 98% HCO3¯22 - 26 mEq/L Base excess -2.0 to 2.0 mEq/L ** Age-dependent
Types of Acids in the Body -Volatile acids: Pco2 is most important factor in pH of body tissues. -Fixed Acids. Catabolism of amino acids, nucleic acids, and phospholipids -Organic Acids: Byproducts of aerobic metabolism, anaerobic metabolism , during starvation, and diabetes. Lactic acid, ketones
Compensation=Buffer Systems Attempt to return the pH to normal or near normal Provide or remove H+ and stabilize the pH. Include weak acids that can donate H+ and weak bases that can absorb H+.
Compensation -If the non primary system is in the normal range (CO2 35 to 45) (HCO3 22-26), then that system is not compensating for the primary. For example: In respiratory acidosis (pH<7.35, CO2>45), if the HCO3 is >26, then the kidneys are compensating by retaining bicarbonate. If HCO3 is normal, then not compensating.
Acid-base Terminology • Acidemia: blood pH < 7.35 • Acidosis: a primary physiologic process that, occurring alone, tends to cause acidemia. • Examples: metabolic acidosis from decreased perfusion (lactic acidosis); respiratory acidosis from hypoventilation. • Alkalemia: blood pH > 7.45 • Alkalosis: a primary physiologic process that, occurring alone, tends to cause alkalemia. • Examples: metabolic alkalosis from excessive diuretic therapy; respiratory alkalosis from acute hyperventilation.
Primary Acid-base Disorders Respiratory Acidosis Respiratory Alkalosis Metabolic Acidosis Metabolic Alkalosis
Primary Acid-base Disorders:Respiratory Acidosis • Respiratory acidosis - A primary disorder where the first change is an elevation of PaCO2, resulting in decreased pH. • Compensation (bringing pH back up toward normal) is a secondary retention of HCO3 by the kidneys; this elevation of HCO3- is not metabolic alkalosis since it is not a primary process. Primary Event Compensatory Event HCO3- ↑HCO3- ↓ pH ~ --------- ↓ pH ~ --------- ↑PaCO2 ↑PaCO2
Respiratory Acidosis Mechanism Hypoventilation or Excess CO2 Production Etiology Pnumonia,Pneumothorax ARDS Respiratory Center Depression Inadequate mechanical ventilation Sepsis or Burns Neuromuscular Disease
Respiratory Acidosis (cont) Symptoms Breathlessness,Restlessness Lethargy and disorientation Tremors, convulsions, coma Skin warm and flushed due to vasodilation caused by excess CO2 Treatment Treat underlying cause Support ventilation Correct electrolyte imbalance .
Primary Acid-base Disorders: Metabolic Acidosis • Metabolic acidosis - A primary acid-base disorder where the first change is a lowering of HCO3-, resulting in decreased pH. • Compensation (bringing pH back up toward normal) is a secondary hyperventilation; this lowering of PaCO2, Renal excretion of hydrogen ions & K+ exchanges Primary Event Compensatory Event ↓ HCO3-↓HCO3- ↓ pH ~ ------------ ↓ pH ~ ------------ PaCO2 ↓PaCO2
Metabolic Acidosis (cont) Symptoms Kussmaul’s respiration Lethargy, confusion, headache, weakness Nausea and Vomiting Lab: pH below 7.35 Bicarb less than 22 Treatment treat underlying cause monitor ABG, I&O, VS, LOC Sodium Bicarb?
Metabolic Acidosis Etiology Conditions that increase acids (lactic acid or ketones) Renal Failure DKA Starvation Lactic acidosis Loss of bicarbonate through diarrhea or renal dysfunction Accumulation of acids Failure of kidneys to excrete H+
Anion Gap Metabolic acidosis is conveniently divided into elevated and normal anion gap (AG) acidosis. AG = Na+ - (Cl- + HCO3) Normal AG is typically 12 ± 4 mEq/L. If AG is calculated using K+, the normal AG is 16 ± 4 mEq/L
Metabolic acidosis and the anion gap 2. Increased gap 1. Normal gap 1. Acid prod 2. Acid elimination Renal “HCO3” losses 2. GI “HCO3” losses Renal disease Lactate DKA Ketosis Toxins Alcohols Salicylates Iron Proximal RTA Distal RTA Diarrhea
MUDPILES • M • U • D • P • I • L • E • S
Primary Acid-base Disorders: Metabolic Alkalosis • Metabolic alkalosis - A primary acid-base disorder where the first change is an elevation of HCO3-, resulting in increased pH. • Compensation is a secondary hypoventilation (increased PaCO2), Compensation for metabolic alkalosis is less predictable than for the other three acid-base disorders. Primary Event Compensatory Event ↑HCO3-↑HCO3- ↑ pH ~ ------------ ↑ pH ~ --------- PaCO2↑PaCO2
Metabolic Alkalosis Risk Factors/Etiology Acid loss due to vomiting gastric suction Loss of potassium due to steroids diuresis Antacids (overuse of)
Metabolic Alkalosis (cont) Symptoms Hypoventilation (compensatory) Dysrhythmias, dizziness Paresthesia, numbness, tingling of extremities Hypertonic muscles, tetany Lab: pH above 7.45, Bicarb above 26 CO2 normal or increased w/comp Hypokalmia, Hypocalcemia Treatment treat underlying cause I&O, VS, LOC give potassium
Primary Acid-base Disorders:Respiratory Alkalosis • Respiratory alkalosis - A primary disorder where the first change is a lowering of PaCO2, resulting in an elevated pH. • Compensation is a secondary lowering(excreting)HCO3 by the kidneys. Primary Event Compensatory Event HCO3-↓HCO3- ↑pH ~ ------- ↑ pH ~ -------- ↓ PaCO2 ↓PaCO2
Respiratory Alkalosis Etiology Hyperventilation due to Conditions that stimulate respiratory center extreme anxiety, stress, or pain Fever overventilation with ventilator hypoxia salicylate overdose hypoxemia (emphysema or pneumonia) CNS trauma or tumor
Respiratory Alkalosis (cont) Symptoms Tachypnea or Hyperpnea Complaints of SOB, chest pain Light-headedness, syncope, coma, seizures Numbness and tingling of extremities Difficult concentrating, tremors, blurred vision Weakness, paresthesias, tetany Lab findings pH above 7.45 CO2 less than 35
Respiratory Alkalosis (cont) Treatment Monitor VS and ABGs Treat underlying disease Assist patient to breathe more slowly breathe in a paper bag or apply rebreather mask Sedation
Metabolic Acid-base Disorders: summary METABOLIC ACIDOSIS↓HCO3- & ↓pH - Increased anion gap • lactic acidosis; ketoacidosis; drug poisonings (e.g., aspirin, ethylene glycol, methanol) - Normal anion gap • diarrhea; some kidney problems (e.g., renal tubular acidosis, interstitial nephritis) METABOLIC ALKALOSIS↑ HCO3- & ↑pH • Chloride responsive (responds to NaCl or KCl therapy): contraction alkalosis, diuretics, corticosteroids, gastric suctioning, vomiting • Chloride resistant: any hyperaldosterone state (e.g., Cushing’s syndrome, Bartter’s syndrome, severe K+ depletion)
Respiratory Acid-base Disorders:summary RESPIRATORY ACIDOSIS↑PaCO2 & ↓pH Central nervous system depression (e.g., drug overdose) Chest bellows dysfunction (e.g., Guillain-Barré syndrome, myasthenia gravis) Disease of lungs and/or upper airway (e.g., chronic obstructive lung disease, severe asthma attack, severe pulmonary edema) RESPIRATORY ALKALOSIS↓PaCO2 &↑pH Hypoxemia (includes altitude) Anxiety Sepsis Any acute pulmonary insult (e.g., pneumonia, mild asthma attack, early pulmonary edema, pulmonary embolism)
Mixed Acid-base Disorders are Common • In chronically ill respiratory patients, mixed disorders are probably more common than single disorders, e.g., RAc + MAlk, RAc + Mac, Ralk + MAlk. • In renal failure (and other conditions) combined MAlk + MAc is also encountered. • Always be on the lookout for mixed acid-base disorders. They can be missed!
Expected changes in pH and HCO3- for a 10-mm Hg change in PaCO2 resulting from either primary hypoventilation (respiratory acidosis) or primary hyperventilation (respiratory alkalosis): ACUTE CHRONIC • Resp Acidosis pH ↓ by 0.07 pH ↓ by 0.03 HCO3-↑ by 1* HCO3-↑ by 3 - 4 • Resp Alkalosis pH ↑ by 0.08 pH ↑ by 0.03 HCO3-↓ by 2 HCO3-↓ by 5 * Units for HCO3- are mEq/L
Predicted changes in HCO3- for a directional change in PaCO2 can help uncover mixed acid-base disorders. • A normal or slightly low HCO3- in the presence of hypercapnia suggests a concomitant metabolic acidosis, e.g., pH 7.27, PaCO2 50 mm Hg, HCO3- 22 mEq/L. Based on the rule for increase in HCO3- with hypercapnia, it should be at least 25 mEq/L in this example; that it is only 22 mEq/L suggests a concomitant metabolic acidosis. b) A normal or slightly elevated HCO3- in the presence of hypocapnia suggests a concomitant metabolic alkalosis, e.g., pH 7.56, PaCO2 30 mm Hg, HCO3- 26 mEq/L. Based on the rule for decrease in HCO3- with hypocapnia, it should be at least 23 mEq/L in this example; that it is 26 mEq/L suggests a concomitant metabolic alkalosis.
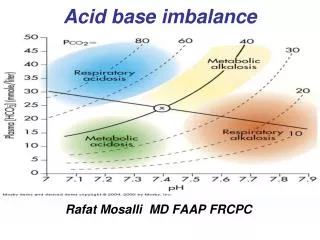
Diagnosis of Acid-Base Imbalances 1. Look at the pH is the primary problem acidosis (low) or alkalosis (high) 2. Check the CO2 (respiratory indicator) is it less than 35 (alkalosis) or more than 45 (acidosis) 3. Check the HCO3 (metabolic indicator) is it less than 22 (acidosis) or more than 26 (alkalosis) 4. Which is primary disorder (Resp. or Metabolic)? If the pH is low (acidosis), then look to see if CO2 or HCO3 is acidosis (which ever is acidosis will be primary). If the pH is high (alkalosis), then look to see if CO2 or HCO3 is alkalosis (which ever is alkalosis is the primary). The one that matches the pH (acidosis or alkalosis), is the primary disorder.
4. Look at the value that doesn’t correspond to the observed pH change. If it is inside the normal range, there is no compensation occurring. If it is outside the normal range, the body is partially compensating for the problem. 37
Case Study #1 HPI: A 5 month-old girl presents with a one day history of irritability and fever. Mother reports three days of “bad” vomiting and diarrhea. Home meds: Acetaminophen and ibuprofen for fever PE: BP 70/40, HR 200, R 60, T38.3 C. Irritable, sunken eyes and fontanelle, skin feels like Pillsbury Dough Boy
Case Study #1 Place IV line Bolus 40 ml/kg of isotonic saline Reassessment (HR 170, RR 40, BP 75/40) Serum studies Sodium 164 mEq/L BUN 75 mg/dL Chloride 139 mEq/L Creatinine 3.1 mg/dL Potassium 5.5 mEq/L Glucose 101 mg/dL Bicarbonate 12 mEq/L pH 7.07 pCO2 11 pO2 121 HCO3 8
Case Study #1 What is the most likely explanation of this patients acidosis?
Case Study #1Metabolic acidosis and the anion gap Anion Gap [Na+] – ([HC03-] + [Cl-]) 164 - (12+139 ) = 13
Case Study #2Metabolic acidosis and the anion gap 2. Increased gap 1. Normal gap 1. Acid prod 2. Acid elimination Renal “HCO3” losses 2. GI “HCO3” losses Renal disease Lactate DKA Ketosis Toxins Alcohols Salicylates Iron Proximal RTA Distal RTA Diarrhea
Summary: Clinical and Laboratory Approach to Acid-base Diagnosis • Determine existence of acid-base disorder from arterial blood PH Check serum HCO3,CO2; if abnormal, there is an acid-base disorder. If the anion gap is significantly increased, there is a metabolic acidosis. • Examine pH, PaCO2, and HCO3- for the obvious primary acid-base disorder and for deviations that indicate mixed acid-base disorders
Summary: Clinical and Laboratory Approach to Acid-base Diagnosis (cont.) • Use a full clinical assessment (history, physical exam, other lab data including previous arterial blood gases and serum electrolytes) to explain each acid-base disorder. • Treat the underlying clinical condition(s); this will usually suffice to correct most acid-base disorders. Clinical judgment should always apply
Acid-base Disorders: Test Your Understanding State whether each of the following statements is true or false. a) Metabolic acidosis is always present when the measured serum CO2 changes acutely from 24 to 21 mEq/L. b) In acute respiratory acidosis, bicarbonate initially rises because of the reaction of CO2 with water and the resultant formation of H2CO3. c) If pH and PaCO2 are both above normal, the calculated bicarbonate must also be above normal. d) An abnormal serum CO2 value always indicates an acid-base disorder of some type. e) The compensation for chronic elevation of PaCO2 is renal excretion of bicarbonate. f) A normal pH with abnormal HCO3- or PaCO2 suggests the presence of two or more acid- base disorders. g) A normal serum CO2 value indicates there is no acid-base disorder. h) Normal arterial blood gas values rule out the presence of an acid-base disorder.
Acid-base Disorders: Test Your Understanding - Answers a) false b) true c) true d) true e) false f) true g) false