Understanding Youth Suicide: Myths, Facts, and Prevention Strategies
420 likes | 526 Vues
This presentation by Dr. Janet McCord discusses the critical issue of youth suicide, outlining its prevalence, risk factors, and protective factors. Highlighting key statistics, such as suicide being the third leading cause of death among 15-24 year olds, it emphasizes the need for effective school-based suicide prevention programs. The session addresses common myths about suicide, warning signs for intervention, and the influence of various social and psychological factors. Attendees will gain valuable insights on how to recognize at-risk behaviors and empower youth with support and resources.

Understanding Youth Suicide: Myths, Facts, and Prevention Strategies
E N D
Presentation Transcript
Wisconsin’s Experience: School-Based Programs for Suicide Prevention Janet McCord, PhD, FT Marian University National Alliance for Grieving Children Conference Phoenix, AZ, June 20, 2013
Discuss the nature of youth suicide: the myths and facts, risk and protective factors, warning signs and appropriate steps for prevention and intervention
In General . . . • Third leading cause of death for 15-to-24 year olds • Second leading cause of death in college students • 50-200 suicide attempts for every completion • Almost 7% of high school students report making a suicide attempt • Over 14% of high school students report suicidal thoughts • Suicide is often linked with drug and alcohol use
General youth suicide rates • Higher among White than among Black • All forms of violent death among Black youth have risen in past 20 – 25 years • Hispanic populations are at high risk for violent death but rates of suicide are lower than for White youth • Native Americans are very high risk for alcoholism, violent death, and suicide • Rate consistently higher than 20/100,000 for all years but one since 1980, and on average more than twice that for all 15-24 year olds • Great variation in rates between tribal groups, geography, and reservation
Gender • Ratio of male to female suicides, age 15-19 • 1970: 3 to 1 • 2000: 4.7 to 1 • Females have higher attempt rates • Males have higher death rates • Numbers of males dying by suicide has risen • Internationally, great variance • Maris, Berman & Silverman (2000): • Males have higher alcohol abuse, access to firearms, shame at failure • Unable to engage in protective behaviors
When • Across all ages, most suicides occur between March and September • December has fewest recorded suicides per day • Rates tend to dip before and during holidays and rise afterwards • Monday is the most common day of the week • Majority of youth suicide occurs in afternoon or evening
Where • Most youth suicides occur at home • Majority of youth suicides involve firearms stored in the home • Case control studies document that presence of a gun in the home substantially increases the risk of suicide (Brent et al, 1993) • Presence of a gun in the home can increase the risk of suicide as much as 75 times that of youth who live in a home without guns (Rosenberg, Mercy & Houk, 1991) • Majority of nonfatal youth suicide attempts involve medications stored in the home
How • Suicidal behavior is a function of psychological intention which is linked to choice of mechanism • Especially true of planned (versus impulsive) suicides • Other factors that influence choice of method • Accessibility and readiness for use • Knowledge, experience, familiarity • Meaning, symbolism and cultural significance • State of mind of person at risk
The problem of attempts • Difficult to measure • Mandated in Oregon • Majority of attempts are low in lethality and no medical assistance is needed or sought • Data based on self-report surveys • Centers for Disease Control and Prevention has monitored nonfatal suicidal behaviors among nationally representative samples of high school students in the biannual Youth Risk Behavior Surveys • Standardized survey • Large sample sizes of 12,000 to 16,000 students • Two questions address suicidal ideation • Two questions address suicide attempts
Attempt to Completion Ratios • Spicer, RS & Miller, TT (2000): Suicide acts in 8 states: Incidence and case fatality rates by demographics and method. American Journal of Public Health, 90, 1885-1891. • 15-19 yo: 101:1 • 10-14 yo: 208:1 • 20-24 yo: 65:1
Variables in Youth Suicide • Social • Psychological • Neurobiological • Genetic • Context of adolescence
Developmental Context • Adolescence a difficult time in life • Conflicts with parents • Mood disruptions • Risk behaviors • Major developmental theorists • Integrative theories • Conceptualization of death
Risk Factors • Psychiatric diagnosis • Avoid singular focus on psychiatric diagnosis • Examine broader psychological characteristics such as cognitive, behavioral, emotional and environmental factors • Mood, substance abuse and conduct disorders • Relation of nondepressed to depressed suicidal adolescents is 660:1 • Substance abuse histories noted in 15% to 30% of teen suicide deaths • In some studies, 70% of teen suicide deaths exhibited some sort of antisocial behavior • Attempts and lethality increase with degree of comorbidity
Other Risk Factors • LGBTQ and Suicide: Some research suggests that there is a link between homosexuality and increased suicidality • No empirical evidence has clearly linked completed suicide to sexual orientation (up to 2007) • Clusters: Adolescents are susceptible to suggestion. A disturbed youth may find the attention given a suicide as desirable.
Protective Factors • More than just the absence of risk factors • Substantial proportion of people with risk factors fail to become suicidal. Why? • Work in this area increasing • Could include: • Adaptable temperament • Internal locus of control • Self-confidence and self-efficacy • Good problem solving skills • Good social support and networks • Good emotional relationship with at least one person in family • Good school experiences • Spiritual faith
Discuss what Prevent Suicide Wisconsin has done to bring effective suicide prevention to individual communities in a predominantly rural state.
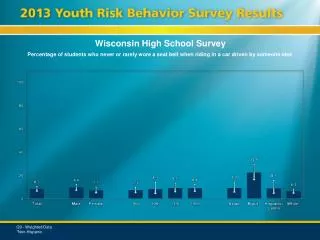
Leading Causes of Death for Wisconsin Youth Suicideis the 2nd leading cause of death for ages 5-19. DHS WISH 2010 Injury Mortality Module (Accessed 03/12)
Wisconsin Youth Suicides 2000-2010 Suicideis the 2nd leading cause of death for ages 5-19. DHS WISH, Injury Mortality Module (Accessed 03/12)
Suicide Rate per 100,000 Youth (age 0-19) Wisconsin US 6.00 6.00 5.50 5.50 5.00 5.00 4.50 4.50 4.00 4.00 3.50 3.50 3.00 3.00 2.50 2.50 2.00 2.00 1.50 1.50 1.00 1.00 0.05 0.05 0.00 0.00
Wisconsin DPI • Curriculum • Dedicated to high quality prevention education and technical assistance • Statewide trainings • 24 minute webinar on the curriculum • Gatekeeper training • Resources http://sspw.dpi.wi.gov/sspw_suicideprev • Wisconsin Safe and Healthy Schools Center • Technical assistance • http://www.wishschools.org/
Classroom Curriculum • Developed by Jon Hisgen, Health and Physical Education consultant • Based on best practices • Grades 6-8 • Grades 8-10 • Week-long set of lessons • Essential knowledge and skills • Built-in assessment component • Experiential learning
What is your depression/suicide IQ? • S.O.S. It’s time to ACT • Phone Booth: scripts related to suicide warning signs • LIGHTS! CAMERA! ACTION! • Review games • Practice lesson for ACT • Demonstrate skills and knowledge related to suicide prevention
Videos • Videos used from Mental Health Screenings SOS Signs of Suicide® Prevention Program • SAMSHA’s National Registry of Evidence-based Programs and Practices • ACT® technique (Acknowledge, Care, Tell) • Trailers
Lifelines Curriculum • Maureen Underwood, John Kalafat, et al. • Maine Youth Suicide Prevention Program • Published by Hazelden • Comprehensive prevention/ intervention/ postvention • Listed in NREPP - National Registry of Evidence Based Programs and Practices of the Suicide Prevention Resource Center • One of the first in the United States • Used by some Wisconsin schools • Polk County
Lifeline Program Components • Administrative readiness • Training for school faculty and staff • Parent workshop • Student curriculum • 4 45-minute sessions or 2 90-minute sessions • Research based • Focus not mental-health based but emphasizes help-seeking and peer support behaviors • Based on Social Development Strategy and Interactive Teaching
Training is important • Teaching about suicide must be voluntary • Teacher is the most important piece • Classroom sessions are flexible • Consider substitute content carefully • Make sure all is interactive • Classroom lessons cannot stand alone • Do not just implement curriculum without the other training pieces for staff and parents • Sensitivity important (to those who have been touched by suicide) • What if? • If community has been affected, wait a semester • Good postvention is excellent prevention
Session One • Introduction, create a safe atmosphere • 12 youth suicides every 24 hours • How know someone? Who does a teen talk to first? Suicide is everyone’s business • Personal reactions • Read a scenario, “what would I do?” and discussion • Reach out • Tell an adult • Not all secrets the same • Information on suicide • Quiz • Myths and facts • Language
Session Two • Warning signs • F.A.C.T.S. • Feelings, Actions, Changes, Threats, Situations • DVD (20 minutes) • 4 role plays, handouts, “what did you observe?” • What to do/not do • Guided practice • Finding the words to show you care • Asking about suicide • Convincing friend to ask for help
Session Three • How to apply the 3 steps • DVD: One Life Saved (7 minutes) • Apply F.A.C.T.S. in discussion to DVD • Protective factors • T.J. had friends that cared; could communicate • Reactions of the friend • Accused of overreacting; weren’t friends anymore • How did the boys feel after they helped T.J? • Proud; happy • Qualities of helpful people • School’s preparedness to help
Session Four • Guided practice through scripted role-plays • Warning signs and suicidal person’s resistance to help • Helper completing an intervention • Emphasizes • Keeping suicidal ideation a secret is dangerous • Recognizing limits and getting help is a good thing • Three steps (care, ask, help) • Help-seeking pledge • Identify 3 people you can turn to for help • Wrap-up • Wallet cards
Conclusion • Youth suicide continues to be a problem • Many suicides are preventable • Schools need to step up and educate • Many curricula exist • Individual schools make decisions regarding crisis team interventions, policies, education
References • http://www.cdc.gov/ViolencePrevention/suicide/statistics/aag.html#D • http://www.cdc.gov/HealthyYouth/yrbs/index.htm • Jobes, DA & Berman, AL (1984). Response bias and the impact of psychological autopsies on medical examiner’s determination of mode of death. Paper presented at the annual meeting of the American Association of Suicidology, Anchorage, AK, 1984 • Goodin, J & Hanzlick, R (1997). Mind your manners. Part II: General results from the National Association of Medical Examiners Manner of Death Questionnaire, 1995. American Journal of Forensic Medical Pathology, 18, 224-227. • Hanzlick, R & Goodin, J (1997). Mind your manners. Part II: General results from the National Association of Medical Examiners Manner of Death Questionnaire, 1995. American Journal of Forensic Medical Pathology, 18 (3), 228-245 • Brent, DA, Perper, JA, Moritz, G, Baugher, M, Schweers, J & Roth, C. (1993) Firearms and adolescent suicide: A community case-control study. American Journal of Diseases of Children, 147, 1066-1071.
Rosenberg, ML, Mercy, JA & Houk, VN (1991). Guns and adolescent suicides. Journal of the American Medical Association, 266, 2989-2995 • Maris, Berman & Silverman (2000). Comprehensive Textbook of Suicidology. New York: Guilford Press • Shenassa, ED., Catlin, SN & Buka, SL (2003). Lethality of firearms relative to other suicide methods: A population based study. Journal of Epidemiology and Community Health, 57, 120-124 • Spicer, RS & Miller, TT (2000): Suicide acts in 8 states: Incidence and case fatality rates by demographics and method. American Journal of Public Health, 90, 1885-1891. • Underwood, M & Kalafat, J. (2009). Lifelines : A Suicide Prevention Program. Center City, MN: Hazelden