Download
1 / 64
670 likes | 1.09k Vues
DISEASES OF KIDNEY AND URINARY TRACT. Lecture on pathomorphology for the 3-rd year students by T. Filonenko. Syndromes of renal diseases. Acute nephritic syndrome The nephrotic syndrome Asymptomatic hematuria or proteinuria Acute renal failure Chronic renal failure

E N D
DISEASES OF KIDNEY AND URINARY TRACT Lecture on pathomorphology for the 3-rd year students by T. Filonenko
Syndromes of renal diseases • Acute nephritic syndrome • The nephrotic syndrome • Asymptomatic hematuria or proteinuria • Acute renal failure • Chronic renal failure • Renal tubular defects • Urinary tract infection • Nephrolitiasis 1
Causes of the nephritic syndrome: • all diffuse-proliferative glomerulonephritis syndromes • post-streptococcal glomerulonephritis • bacterial endocarditis • lupus • mild / early RPGN syndromes • anti-GBM (Goodpasture's, other) • Wegener's • polyarteritis • bad IgA-family (Berger's, Henoch-Schonlein, etc.) • membranoproliferative glomerulonephritis 3
Causes of the nephrotic syndrome • amyloidosis • diabetic glomerular disease • foot process disease • minimal change glomerulopathy • focal-segmental glomerulosclerosis • membranous glomerulopathy • membranoproliferative glomerulonephritis • birth defects 5
Glomerular diseases Named diseases (by service pathologists): - Diseases that primarily involve the glomerulus (acute post-streptococcal glomerulonephritis, etc.) - Systemic disease in which there are glomerular changes (systemic lupus, amyloidosis, diabetes, Goodpasture's syndrome, etc.) 7
Principles of glomeluronephritis classification • Gomerulonephritis may be primary or secondary. • According to the etiology it may be bacterial, viral, unclear. • According to the pathogenesis there are 2 types of glomeluronephritis: immuno- associated and non-immunoassociated. • According to the course GN may be classified into acute, sub-acute, chronic. • Histologic and ultrastructural appearance of injury (by light and electron microscopists). • According to topography: inter- and extracapillary GN. • According to character of inflammation: nonsuppurative exudative and proliferative. • According to propagation: diffuse and local. 8
MECHANISMS OF GLOMERULAR INJURY Immune: • In situ immune complex formation • Circulating immune complex deposition Nonimmune: • Metabolic glomerular injury (diabetic nephropathy) • Hemodynamic glomerular injury (systemic hypertension) • Deposition diseases (cryoglobulinaemia, amyloidosis) • Infectious diseases (HBV, HCV, HIV) • Inherited glomerular diseases(Alport’'s syndrome). 9
HISTOLOGIC ALTERATIONS IN GLOMERULAR DISEASE • Cellular proliferation (intra- and extracapilary) • Leukocyte infiltration • Visceral epithelial cell swelling and detachment • Glomerular basement membrane thickening • Hyalinosis • Mesangiolysis • Necrosis 10
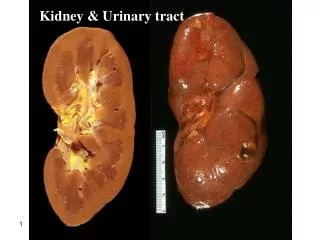
Acute poststreptococcal glomerulonephritis • This disease may follow several weeks after infection with certain strains of group A beta hemolytic streptococci. • This produces the nephritic syndrome. • Patients typically have an elevated anti-streptolysin O (ASO) titer and decreased C3 levels in the serum. • The cause is deposition of circulating immune complexes which fix complement and attract PMN's • In occurs most frequently in children of six to ten years of age, but adults of any age can be affected. • Duration of disease from 1.5 to 12 months. • Gross appearance: Kidney enlarged; cortex broad, pale, without markings; medullary rays congested; glomeruli just visible as grey avascular dots. 12
The hypercellularity of post-streptococcal glomerulonephritis • Proliferation of endothelial, mesangial and epithelial cells; • Infiltration by leukocytes; The proliferation and leukocytes infiltration are diffuse; • Swelling of endothelial cells; • Obliteration the capillary lumen 13
Electron microscopy shows these granules to be large, dense, hump-shaped deposits located subepithelially 14
Glomerulus, crescentic glomerulonephritis, PAS stain Large crescent Notice the fibrin in the crescent that has escaped from the severely damaged and broken glomerular basement membrane (GBM). 18
Glomerulus, IgA nephropathy, PAS stain 22
By electron microscopy in membranous glomerulonephritis, the darker electron dense immune deposits are seen scattered within the thickened basement membrane. 24
Membranous glomerulonephritis, silver stain Capillary loops Mesangial areas 26
Minimal change disease (MCD) (Lipoid nephrosis) • Nephrotic syndrom in children can be often; characterized by normal glomeruli on light microscopy but uniform and diffuse effacement of the foot processes of visceral epithelial cells on electronic microscopy. • GBM isn’t changes. • Tubules are dilated; their epithelium is swelling, containing hyaline and fatty droplets. • Fatty degeneration, necrobiosis, atrophy, desquamation in tubular epithelium take place. • Gross appearances (“big white kidneys”): kidneys enlarged, flabby, yellow color. 28
Minimal change disease (MCD), silver stain Podocytes CL 29
Minimal change disease (MCD), trichrome stain Tubular lipoid cells 30
Focal segmental glomerulosclerosis (FSGS) Hematoxylin and eosin Trichrome stain 33
Focal segmental glomerulosclerosis (FSGS) 1 3 2 1- segmental sclerosis 2- interstitial inflammation 3- Atrophic tubules 34
Membranoproliferative glomerulonephritis Notice the lobular pattern, the hypercellularity, and the collapse of the capillaries. 37
Membranoproliferative glomerulonephritis (MPGN), later stage, silver stain At a later stage of MPGN, many of the capillary loops show a double contour, or "tram-track," appearance 38
This electron micrograph demonstrates the dense deposits in the basement membrane of MPGN. 39 21
Chronic glomerulonephritis (CGN) • CGN is the final stage of GN when sclerosis has eliminated many glomeruli and their associated tubules. • Light microscopy shows hyaline obliteration of glomeruli, transforming them into acellular hyaline masses made of mesangial matrix, basement-membrane material, dense collagen, and trapped plasma protein. • Tubules are lost, vessel walls are thickened, and ultimately the kidney is totally destroyed. • Given the usual trans-stygian kidney, the pathologist cannot even tell whether the original disease was glomerular, interstitial, or vascular. 40
Gross appearance: • The kidneys are symmetrically contracted and have diffusely granular, cortical surfaces. • Pieces of renal tissue adhere to stripped capsule; capsule is adherent and strips with difficult. • Weight is 50 gm each. • On section, the cortex is thinned and irregular,pelvis dilated and they’re in an increasing peripelvic fat. • Such kidneys are called “secondary shrinkage kidneys” 41 25
This is nodular glomerulosclerosis. Nodules of pink hyaline material form in regions of glomerular capillary loops in the glomerulus. 42 27
Kidney failure: loss of renal function. • Acute renal failure usually presents as oliguria (less than 500 mL urine/day) plus azotemia. Hyperkalemia is the main threat to life during the oliguric phase. • Chronic renal failure is the end result of irreversible kidney damage from any cause. 43
Acute renal failure and acute tubular necrosis.Acute renal failure (ARF) is a syndrome associated with acute suppression of renal function, often accompanied by oliguria, and rarely anuria or polyuria. ARF is caused by: • Organic vascular obstruction. • Severe glomerular disease. • Acute tubulointerstitial nephritis • Massive infection • Disseminated intravascular renal coagulation • Urinary obstructions • Acute tubular necrosis 44 29
Acute tubular necrosis (ATN). • ANT is characterized by destruction of renal tubular epithelial cells either from ischemia or nephrotoxins. • Ischemic ATN is called tubulorrhectic ATN or shock kidney, occurs due to hypoperfusion of the kidneys resulting in focal damage to the tubules. • Nephrotoxic ATN occurs as a result of direct damage to tubular cells by ingestion, injection or inhalation of a number of toxic agents. 45 30
The clinical course of ATN may be deviled into stages: 1. The initiating stage (shock), lasting for about 36 hours, is dominated by the inciting medical, surgical, or obstetric event in the ischemic form of ATN. Macroscopically, kidneys are diffusely swollen and edematous. It is characterized by ischemic cortex and congestion of pyramids. Acute renal failure and oliguria, hyperkalemia and fluid overload in patients develop. 35
2. The maintenance stage (Oliguric phase, 2-9 days) is characterized by sustained decreases in urine output to between 40 to 400 ml per day, with salt and water overload, rising blood urea nitrogens, hyperkaliemia, metabolic acidosis, and other manifestations of uremia dominating this phase. There is blockage of renal tubules by necrotic cells, and a secondary reduction in glomerular blood flow (caused by arteriolar constriction) reduces glomerular filtration. It stage may be fatal. 36
3. The recovery stage (Polyuric phase, 10-21 days) is ushered by a steady increase in urine volume that may reach up to 3 liters per day. Regeneration of renal tubular epithelium takes place, with removal of dead material by phagocytic cells, as well as in the form of casts in urine. As tubules open up and glomerular blood flow increases, patients develop polyuria. This is because the regenerated tubular cells are undifferentiated and have not developed the specializations necessary for resorption of electrolytes and water. Replacement of fluid and electrolytes is needed to compensate for excessive loss from urine. Hypokalemia, rather than hyperkalemia, becomes a clinical problem. 37