Download

1 / 16
160 likes | 253 Vues
Global Agenda on Medicines. Health Research in the South. Daniel Maceira, Ph.D. danielmaceira@cedes.org www.danielmaceira.com.ar. Objectives. Propose a Framework to Analyze Research Priorities in Health and Pharmaceuticals in Developing Nations.

E N D
Global Agenda on Medicines. Health Research in the South Daniel Maceira, Ph.D. danielmaceira@cedes.org www.danielmaceira.com.ar
Objectives • Propose a Framework to Analyze Research Priorities in Health and Pharmaceuticals in Developing Nations. • Provide Results about Research Projects funded by National Governments in Latin America (Argentina, Bolivia, Chile, Paraguay, Uruguay). • Identify Priority Setting Mechanisms for Health Research within a Framework of National Innovation Systems • Analyze the Presence of Coordination between Public Funding & Research Institutions in Argentina. • Discuss Specific Research Lines Developed on Pharmaceuticals under the new Argentine Macro and Institutional Context. • Suggest Principles to Include in a Collaborative Agenda.
TwinTheoretical Frameworks Health Care Goods and Services Provision System Innovation System • Needs: rights and financing mechanisms. • Improve efficiency and increase allocative equity. • Generate knowledge: public goods and appropriability. • Reduce access gap and cover R&D needs. • Asymmetric Information (physician / researcher) • Incomplete Information (prob. illness / invention) • Externalities • Unequal bargaining power among parties. • The market exchange mechanisms are inefficient in both cases: It requires an intervening State (regulation, financing, provision of health goods and services).
Health System National Innovation System Innovation Health System Theoretical Framework: Health Research National Innovation System Analysis of the flow of funds from the viewpoint of the supply Definition: “The network of institutions of the public and private sector whose activities and interactions initiate, import and disseminate new technologies” (Freeman, 1987). • Functions: • Provision of Research and Development (R&D), creation of new knowledge on new products, new process, new managerial techniques to improve health Status . • Creation of human capital, production and reproduction of skills to be used in R&D activities. Primary and Secondary Technology Generation (Katz, 1976) • Creation and change of the needs of the institutions to develop new fields of innovation. Innovation Health System Goal: Create Local Capabilities to Improve Public Decision Making Process in Health and Pharmaceuticals
Basic Conditions Structure Strategy Performance Public Involvement & Priority Setting in Research • Income Distribution Policies • Access to Clean Water and Sanitation • Reforms on Payroll Tax Based Social Insurance Schemes Public Policy • Certification of New Drugs and Plants • Creation of Public Laboratories • Sign PAHO Revolving Fund • Licenses • Generalized Basic Package of Health Services • Price Controls • Prescription of Drugs by Generic Name • Public Purchases of Drugs for the Poor at HCCenters
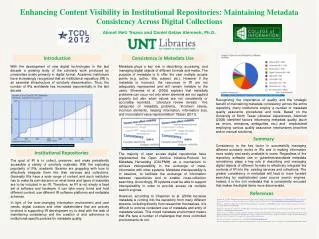
18.0% 16.0% 15.7% 14.9% 14.4% 14.0% 12.0% 11.3% 10.8% 10.0% Total OOP 9.0% 8.7% OOP in Medicines 8.0% 7.6% 6.2% 6.0% 6.0% 5.7% OOP in Health Services 4.6% 4.5% 4.3% 4.0% 3.3% 2.0% 0.0% I II III IV V Income Quintile Argentina: Out of Pocket Health Expenditures, 2003 Equity Gap
Methodology • Building of a database on public funding of health research ("Winning” Cases: supply and prioritization). • Classification of research topics in 27 categories (3 research methodologies and 9 objective categories).
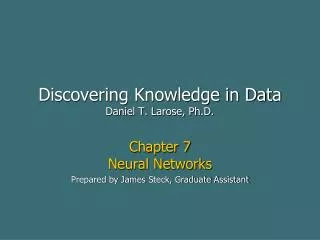
Evolution of Health Research, Public Flows. Millions of US$ PPP. 2002-2006 Source: Maceira et al (2009)
DALYS, by Country. 2004 National Innovation System Health Research Priority Setting: Strategy 1: Direct Investments based on Impact (NonComm. Diseases) Strategy 2: Reduce Equity Gap. Direct Investments to Comm. Diseases Strategy 3: Improve Management and Resource Allocation within Subsystems: Direct Investments to Public Health
Biomedical Objectives Social, Economic and Cultural Communicable Illnesses Non Communicable Illnesses Nutrition and Environment Violence and Accidents Health Policy, Systems & Services Technological R&D Traditional Medicine Basic Science Clinical Objectives Social, Economic and Cultural Communicable Illnesses Non Communicable Illnesses Nutrition and Environment Violence and Accidents Health Policy, Systems & Services Technological R&D Traditional Medicine Basic Science Public Health Objectives Social, Economic and Cultural Communicable Illnesses Non Communicable Illnesses Nutrition and Environment Violence and Accidents Health Policy, Systems & Services Technological R&D Traditional Medicine Basic Science Categories Priorization and Relative Participation on Allocated Resources. 2006 Objectives
Publications per 10.000 inhabitants.Low Productivity Source: Maceira et al (2009)
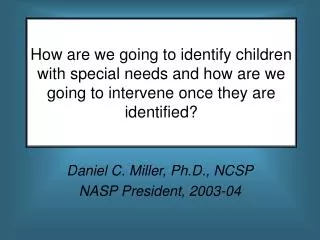
Public Funded Projects by Recipient Institution according to Methodological Category. Argentina, 2002-2006 Source: Based on information provided by ANPCyT, CONICET and Salud Investiga.
Argentina New Macroeconomic & Institutional Context • No Patent Protection on Design. Import Substitution Industry. About 50% of Pharmaceutical Sales belong to Domestic Private Firms, Certified by ANMAT (Local FDA). Hidden Agenda: Avoid Intertemporal Inconsistency (Monopoly-Spread Access to Innovation) • Macroeconomic Crisis (2001): Dramatic Change in Exchange Rates affecting Import and Production Patterns in Pharmaceutical Industry • Wide Variations in Employment Rates affecting Social Insurance Coverage and Access to Medicines • New Patent Protection Law (2003) • Legislation on Prescription by Generic Name (2003) and Changes in Pharma Relative Prices (Brand Reputation & Ability to Switch) • Remediar Program (2002) : Provision to HC Centers of Medicines covering 70% of PHC Needs, Improving Access to the Poor and Reducing OOP Expenditures • Stimulus to Public Production of Pharmaceutical Products
Collaborative Agenda on Pharmaceuticals in Argentina (Examples) • Social Insurance in Provinces (CEDES-Industry-MinHealth) • Efficiency of ANMAT & INPI (CIPPEC-CEDES-Industry) • Household Surveys and Health Expenditures Analysis: 2003- 2005 (CEDES-CIPPEC-Industry) • Health Systems Reforms in Middle Income Countries in Eastern Europe and Latin America (CEDES-Industry) • Remediar Program (IDB-CEDES-MinHealth) • Public Health Essential Functions Project (CEDES-MinHealth) • Superintendence of Social Health Insurance: Creation of Technological Evaluation Office • Project on Catastrophic Expenditures Funds (MinSalud-MinProvSalta-CEDES) • Estimation of Demand Functions for Therapeutic Class & Price Controls (CEDES-Industry) • Impact Estimation of Prescription by Generic Name Law (CEDES-Industry) • Courses and Conferences on Health Economics and Pharmaeconomics • Health Economics for Journalists (CEDES-Industry) • Media Articles – Trigger Public Health Agenda • Research on Key • Topics: • Impact Evaluation: • Research-to-Action • Initiatives: • Impact Regulations: • Training & Advocacy: • Collaboration in Public Policy Design • Clinical Trials & Public Hospitals (>900 in Buenos Aires Public Hospitals)
Research-to-Action Project Implies: • Political Economy of Pharmaceutical Sector (Actors-Objectives-Strategies-Beliefs-Payoffs). • Public Sector: Priority Setting under Budget Constraints, Political Pressures and Urgent Needs. Institutional Capacity and Bargaining Power in Developing Countries. • Patients as Interest Group: no clear representation, discontinuous, uncomfortable as actor. Poor advocacy capacity, specially the poor. • Building Public-Research-Industry Agreements based on Public Priorities on Health Care Policy • Recognition of Each Other’s Objectives & Skills • Acknowledgment of Each Other’s Languages and Priorities • Willingness to Develop a non-Naive Common Ground for Collaboration • Recognition that there will not be “Perfect Alignment” in Goals • Need for Building Long Lasting Relations based on Technical Skills
How do we get there? Requirements • Define Countries/Needs/ Supply Characteristics • Define Policy Goals s.t. a Public Priority Setting Framework • Develop Research Skills in the South within Independent Structures (Research Centers & Universities) • Develop Collaborative Training Programs favoring North-South Exchange of Experiences, Tools and Priorities • Identify Consortia between Multilateral Organizations, Developed Nations’ Agencies, Developing Governments’ Counterparts, Industry, Research Institutes • Define Spaces for Debate and Exchange of Ideas • Define an Advocacy and Communication Agenda