1: Shoulder Dystocia
50 likes | 626 Vues
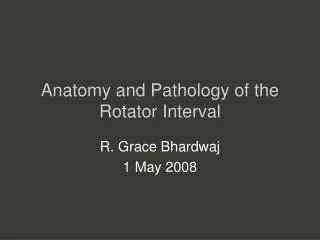
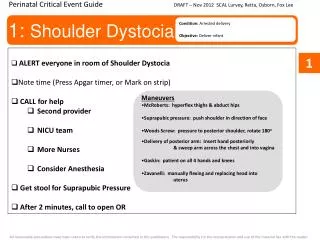
Perinatal Critical Event Guide. DRAFT – Nov 2012 SCAL Lurvey, Retta, Osborn, Fox Lee. 1: Shoulder Dystocia. Condition: Arrested delivery Objective: Deliver infant. ALERT everyone in room of Shoulder Dystocia Note time (Press Apgar timer, or Mark on strip) CALL for help Second provider

1: Shoulder Dystocia
E N D
Presentation Transcript
Perinatal Critical Event Guide DRAFT – Nov 2012 SCAL Lurvey, Retta, Osborn, Fox Lee 1: Shoulder Dystocia Condition: Arrested delivery Objective: Deliver infant • ALERT everyone in room of Shoulder Dystocia • Note time (Press Apgar timer, or Mark on strip) • CALL for help • Second provider • NICU team • More Nurses • Consider Anesthesia • Get stool for Suprapubic Pressure • After 2 minutes, call to open OR 1 • Maneuvers • McRoberts: hyperflex thighs & abduct hips • Suprapubic pressure: push shoulder in direction of face • Woods Screw: pressure to posterior shoulder, rotate 180o • Delivery of posterior arm: Insert hand posteriorly • & sweep arm across the chest and into vagina • Gaskin: patient on all 4 hands and knees • Zavanelli: manually flexing and replacing head into • uterus All reasonable precautions have been taken to verify the information contained in this publication. The responsibility for the interpretation and use of the material lies with the reader.
Perinatal Critical Event Guide DRAFT – Nov 2012 SCAL Lurvey, Retta, Osborn, Fox Lee 3. Eclamptic Seizure Condition: Eclamptic seizure Objective: Stablize mother, monitor fetal heart rate, treat the seizure • Don’t forget your ABCs • Airway (assess and secure) • Breathing (100% FiO2) • Circulation (adequate IV access) • ALERT everyone in room of Seizure • CALL for help • Second provider • Anesthesia • More Nurses • ASSIGN Recorder (Charge Nurse) • If postpartum, secure infant • VITAL SIGNS: BP, O2, Fetal Heart Rate • ABCs • Position airway to keep open, Place oxygen • Position patient on side to prevent aspiration • Monitor Fetal heart rate, Expect a deceleration • Magnesium, 4g loading dose • Antihypertensives • Labetalol 20mg, 40mg, 80mg every 10 minutes, Max 220mg • Hydralazine 5mg, 10mg every 15-20 minutes 3 • Fetal Heart Rate • Expect a deceleration • Stabilize mom first • If bradycardia remains for 3-4 minutes • after seizure resolves, consider C-section All reasonable precautions have been taken to verify the information contained in this publication. The responsibility for the interpretation and use of the material lies with the reader.
Perinatal Critical Event Guide DRAFT – Nov 2012 SCAL Lurvey, Retta, Osborn, Fox Lee 6: Neonatal Resuscitation Condition: Failed airway (2 unsuccessful attempts or oxygen saturation less than 85%). Objective: Establish adequate oxygenation/ventilation. • CALL Code PINK • Start Apgar Timer when baby out • ASSIGN Recorder (Charge Nurse) • Bring in NICU Rapid Response Cart (Green) • Stimulate, warm and dry infant for 30 sec • VITAL Signs: HR, O2 • Not breathing/Grunting or HR <100 • Start bagging baby (Positive Pressure Ventilation) • Make sure Bagging is effective • If not, DON’T MOVE ON. Troubleshoot equipment and seal on baby • Reasses HR and O2 every 30 seconds • If HR < 60, start Chest compressions and continue Bagging • If HR between 60 and 100, Continue Bagging baby • Continue Bagging or compressions until help arrives 6 NRP HR <60 Chest compressions AND PPV HR 60-100 PPV only SpO2 after birth 1 min 60-65% 2 min 65-70% 3 min 70-75% 4 min 75-80% 5 min 80-85% 10 min 85-95% All reasonable precautions have been taken to verify the information contained in this publication. The responsibility for the interpretation and use of the material lies with the reader.
Perinatal Critical Event Guide DRAFT – Nov 2012 SCAL Lurvey, Retta, Osborn, Fox Lee 8: Postpartum Hemorrhage Condition: Acute massive bleeding. Objective: Stop bleeding, maintain hemodynamic stability, avoid coagulopathy and hysterectomy. • ALERT everyone in room of Hemorrhage • CALL for help • Second provider • Anesthesia • More Nurses • ASSIGN Recorder (Charge Nurse) • Secure baby • VITALS – BP, HR, O2, QBL • Hemorrhage Kit/Cart and Bakri Balloon in Room • IV Second Line, Bolus 2 NS or LR (warm fluids or warm patient) • Give Hemostatic agents, only one of each • VITALS Q 5 MINUTES, Call Out and Record • QBL update if bleeding continues • Foley Cath (Record initial amount of urine) • Activate OB Hemorrhage protocol for Blood loss >1500ml or VS changes • After 4 units PRBCs, add 4 units FFP and 1 unit platelets • Bleeding continues: Insert Bakri Balloon • Bleeding continues: Move to OR for surgical intervention • INTERVENTIONS BY PROVIDER • Medications: Pit, Methergine, Misoprostol, Hemabate • Exam, Remove clots • Bakri Balloon • D&C • Consider Interventional Radiology • OR Interventions (B-Lynch, O’Leary, Hysterectomy) • If provider requests labs drawn: • CBC, Lytes, INR/PTT, Fibrinogen, Lactate 8 Consider Causes of PPH TONE: Bakri Balloon or B-Lynch IF ATONY TISSUE: D&C IF Retained Products TRAUMA: Repair of Laceration IF Trauma THROMBIN: Massive Transfusion (recom factor VIIa) IF DIC TRANSFUSION BEGINS - RATIO 4 PRBCS: 4 FFP: 1 PLTS All reasonable precautions have been taken to verify the information contained in this publication. The responsibility for the interpretation and use of the material lies with the reader.