Download
1 / 55
580 likes | 1.18k Vues
Defects of the Genitourinary System. Review of Anatomy and Physiology of the Genitourinary System. The urinary system is composed of: The kidneys, ureter, bladder and urethra.

E N D
Review of Anatomy and Physiology of the Genitourinary System The urinary system is composed of: The kidneys, ureter, bladder and urethra. The kidneys lie outside the peritoneal cavity in the upper posterior portion of the abdominal wall, one on each side. Each kidney is made up of one million functional units, called Nephrons. Water and small molecules are filtered and larger molecules stay in the bloodstream. What results (is left in the kidneys) is filtrate. Approximately 20% of the filtrate is plasma, (no RBC’s, WBC’s, platelets or protein) Substances that pass through are selectively reabsorbed or filtered (Na, Bicarb, K, glucose, creatinine, urea). Filtrate becomes concentrated in the distal tubules and becomes the urine that reaches the renal pelvis
Review of Anatomy and Physiology of the Genitourinary System • Nephrons are the functional units that form urine, there are about 1 million in each kidney. Nephrons are comprised of a glomerulus and a tubule (proximal tubule, loop of Henle, distal tubule). Plasma is filtered across the glomerulus, of the plasma that enters the tubule, only a small fraction is excreted as urine. The Nephrons empty into collecting ducts (tubules) that join to form the pelvis of each kidney. BP determines how fast and under what pressure blood passes through the kidneys, they receive approximately 1 L of blood/min. Blood is supplied to the kidneys via the renal arteries, one to each kidney
Review of Anatomy and Physiology of the Genitourinary System • The main function of the urinary system is to: • Regulate fluids, electrolytes and maintain acid base balance. • Remove metabolic end products (waste) form blood. • Regulate blood pressure.
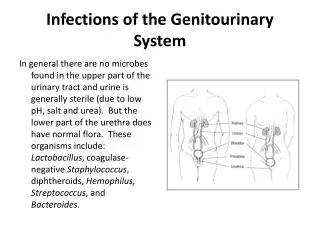
Urinary Tract Infection (UTI) Etiology/ Pathphysiology: • An infection and inflammation anywhere in the urinary tract (including the kidneys), caused by the proliferation of a microorganism, most are bacterial in nature but virus and fungi can also be the cause. The most common organism is Escherichia Coli. (80- 90% in the pediatric population) • Cystitis: An infection of the bladder (most common) • Polynephritis: An infection of the kidney itself (can be an acute infection or chronic infection)
Urinary Tract Infection (UTI) • Urinary Tract Infections (UTI) are more common in girls, ages 7-11, males 2-6 years. Female to male ratio 9:1. The incidence peaks again (in females) during adolescence with sexual activity. • One cause for the increased incidence in females is due to the shorter urethra in the female provides a ready path for organisms and the urethra opening in the vagina is so close to the anus.
Urinary Tract Infection (UTI) • Symptoms of Cystitis include: • Urgency • Increase frequency of urination • Burning on urination • Pain on urination (dysuria) • A sense of urgency to urinate • Nocturia • Pain or spasm in the bladder region, pain in lower back • Pyuria (WBC’s in urine) • Bacteria and RBC’s (found on urinalysis)
Urinary Tract Infection (UTI) • Symptoms of Acute Polynephritis include: • Fever • Chills • Flank pain • Dysuria
Clinical manifestations of UTI Theinfantwith a UTI initially presents with vague symptoms: • Colic • Jaundice • Poor eating • Vomiting • Fever • Lethargy • Irritability • Increased number of wet diapers • FTT
Clinical manifestations of UTI The preschool child presents with: • Fever (most common sign) • Weak urinary stream or dribbling of urine • Hematuria • Abdominal pain • Frequency • Urgency • Dysuria • Incontinence in the toilet trained child
Clinical manifestations of UTI The school aged child presents with: • Diarrhea • Strong smell to urine • Hematuria • Dysuria • Frequency • Urgency
Clinical manifestations of UTI Children of all ages can present with: • Abdominal distension • Dehydration • Flank pain • Costroverterbal angle (CVA) tenderness • Chills and Fever • Constipation
Diagnostic Evaluation Urine analysis (UA) • Done via the clean catch method (mid-stream urine after the child has wiped perineum with a cleansing cloth. • In infant/toddler obtained by “bagging. • Will be a “dirty” specimen and evaluated for ph, presence of ketone, glucose, blood (RBC's). Urine Culture/Urine sensitivity (UC & S) • A sterile specimen, must be obtained by urinary catheterization. • To evaluate the presence of WBC’s, bacteria • Sensitivity will indicate which antibiotic organism is sensitive to.
Diagnostic Evaluation Intravenous pyelogram (IVP) • A radiological procedure done by injecting dye (IV) to visualize the structure of the urinary tract. (kidneys and bladder) Voiding Cystourethrogram (VCUG) • To establish the presence of urinary reflux and other UT abnormalities. Done by placing a Foley and injecting dye into the UT and with a type of x ray used to watch the progression of the urinary flow through the UT.
Causes of UTI in pediatric patient • Anatomical differences in girls • Urinary stasis - holding urine in allows for over growth of bacteria. The bladder is a nice warm place in which bacteria will thrive if left there to long • Contamination from incorrect toileting/cleaning • Irritation from caustic agents (girls-bubble baths) • Structural defects • Reflux • Incomplete voiding (holding) of urine, children tend to leave some behind as they are to busy to stay in the bathroom, encourage double voiding. • Tight fitting clothing or diapers. Diapers are a nice warm breading ground for bacteria.
Treatment of UTI Bacterial UTI is treated with a 7-10 course of PO or IV antibiotics. The most commonly used antibiotics are: Bactrim/Septra, nitrofurantoin, amoxicillin, sulfasoxazole, Cefaclor and ampicillin.
Nursing considerations • Obtain UA & UC & S before starting antibiotics. • Monitor child's response to antibiotics. • Encourage liberal intake of fluids • Repeat UA 48-72 hours after antibiotics have started and 1 week after therapy has ended. • Instruct parents on the importance of completing the complete course of antibiotics.
Nursing considerations • Teach child (age appropriate) to void frequently. • Instruct child and parent about proper cleaning after voiding/stooling (Front-back) • Instruct about the avoidance of bubble baths (esp. in girls) • Encourage the use of cotton underwear (esp. in girls) • Teach the child that they should void the first time the “urge” to void presents, not wait.
Vesicouretral Reflux Urinary reflux is the abnormal retrograde flow of urine into the ureter (urine goes back up ureter towards the kidneys). Reflux itself does not cause UTI but it is associated with a higher risk of Polynephritis. With the presence of reflux , infected urine (a simple UTI or just overgrowth of bacteria) has direct access to the kidneys, the result is usually Polynephritis.
Vesicouretral Reflux Reflux and recurrent febrile UTI (Polynephritis) can cause renal scarring. It is treated in one of two ways: • Surgery to correct any anatomical defect that might be causing the reflux • Low dose prophylaxis with antibiotics, frequent UC & S (every 2-3 months) and every time the child is febrile. A yearly VCUG to assess. Most children will outgrow the reflux within a few years.
Hypospadias A congenital defect in which the urethral opening (urinary meatus) is located on the underside of the penis. It can be located at anywhere on the underside of the penis. Can be associated with chordee, a band of tissue that will pull the penis downward into a curvature. Occurs in 1:300 boys
Treatment and Nursing considerations-Hypospadias. • Child can not be circumcised at birth as the foreskin may be used during surgical repair. Surgery may be done as young as 3 months or as late as 2 years. Will be done in the infant if a chordee is present. • Depending on the severity and exact location of meatus the surgical procedure can be done as an outpatient. • Surgery is successful when the child voids through the newly constructed urethra.
Acute Glomerulonephritis Etiology: an acute inflammation of the glomerulus. It is not an infection of the kidney, but the direct result of an antigen-antibody response to a preceding GABHS infection. It is commonly preceded by a strep pharyngitis/tonsillitis 1-2 weeks prior to the onset of nephritis. (80% of cases) Most common in the 2-6 year age. But can occur in any age group. Can be acute or chronic.
Acute Glomerulonephritis Pathology: exact mechanism of action is unknown, it is believed to be an antibody-antigen type reaction that stimulates IgG (an antibody ,the major immunoglobulin found in serum). This antibody –antigen response creates a membrane type substance that lodges in the glomerulus.
Acute Glomerulonephritis The glomerulus become edematous and infiltrated with leucocytes which in turn occlude the capillary lumen, decreasing the plasma filtration rate leading to an excessive accumulation of H2O and retention of Na that expands interstitial fluid volume and plasma volume, causing circulatory congestion and edema. Hypertension is associated with Glomerulonephritis. In other words the glomerulus became clogged and normal plasma filtration cannot occur and massive edema occurs as fluid is pushed into the intestinal tissue.
Clinical Manifestations of Glomerulonephritis • Child is in their usual state of good health until strep infection. • Has an average 10 day “incubation” period from the time of the initial strep infection to the onset of symptoms. • Initial signs are edema of face, periorbital edema, anorexia and dark urine. • Facial edema is more prominent upon awakening (dependant edema), it then spreads to the abdomen and extremities during the day.
Clinical Manifestations of Glomerulonephritis • UO is decreased • Urine is cloudy, having the color or tea or cola. • Child is pale, irritable and lethargic • moderate – severe hypertension may be present. • The younger child will look ill but seldom have complaints • The older child will c/o headache, abdominal pain • In all ages groups: vomiting, dysuria, anorexia, cough and dyspnea due to pulmonary congestion from fluid retention.
Laboratory findings • UA & UC & S • Proteinuria will be present (1+ - 4+) • Hematuria • Presence of RBC’s • Blood tests • Elevated BUN • Creatinine • Alterations in electrolytes • Metabolic acidosis • Decreased Na & Ca • Increased K+, Ph, albumin • CBC • Mild anemia with drop in Hct
Potential complications • Deteriorating renal function • Significant t hypertension • Significant anemia (most common in the chronic version) • Cardiac failure (due to increased blood volume secondary to retention of Na & H20 which will cause pulmonary congestion).
Treatment There is no specific treatment for Glomerulonephritis, treatment is symptomatic. • Correction of hypertension, with diuretics and or Antihypertensives. • Correction of any electrolyte imbalances
Nursing Care of the child with Acute Glomerulonephritis • Child can be treated at home if BP and UO is normal • The child with significant hypertension, edema, gross hematuria and oliguria need to be hospitalized. • Bed rest is required during the acute phase • Monitoring for fluid & electrolyte imbalances • Antihypertensives and diuretic as ordered • Diet restrictions depend on severity: Na & fluid intake may be restricted to some extent. Foods high in K+ are restricted during periods of oliguria to prevent hyperkalemia. Other wise child can have a normal diet.
Nursing Care of the child with Acute Glomerulonephritis • Strict I & O • Daily weights • Vital signs with BP q4h • Antibiotic therapy in children that show persistent strep • Skin care of edematous areas to prevent skin breakdown. Almost all children recover quickly, and reoccurrence is rare. The child will need follow up visits weekly x 1 month, then monthly for 6 months for routine UA: microscopic hematuria may persist for months.
Nephrotic Syndrome (Nephritis) Etiology: Idiopathic, increased glomerular membrane permeability to plasma protein resulting in: • Proteinuria • Hypoalbuminemia • Hyperlipidemia • Edema Normally the glomeruli are impermeable to albumins and other proteins (esp. albumin which is 60% of the body's protein)
Nephrotic Syndrome (Nephritis) Pathphysiology: Characterized by increased glomerular permeability to plasma protein, resulting in massive urinary protein loss, this increased permeability allows albumin to pass into the urine Tubular reabsorption of Na & H2O is increased, expanding the intravascular volume. Protein deficiency leads to increased osmotic pressure allowing fluids to escape into tissue, massive edema results. Hyperlipidemia is caused by the liver producing more albumin to compensate for losses by synthesing more proteins and lipids. The loss of protein leads to decreased immunoglobulins and increases susceptibility to infection. Incidence is slightly higher in girls than boys. It primarily affects school age children.
Clinical manifestations in the child with Nephrotic syndrome • Previously well child shows increasing weight gain over a period of days or weeks • Fluid retention with generalized severe edema occurs in face, abdomen, genital area, and extremities (onset of edema can be gradual or rapid) • Child becomes anorexic, irritable and lethargic. • Child c/o abdominal pain due to abdominal distension
Clinical manifestations in the child with Nephrotic syndrome • Pallor • Fatigue and activity intolerance • BP is usually normal or lower than normal. • Urine: • Oliguria • Dark & frothy • Contains RBC’s (but no gross hematuria is present). • Massive proteinuria • High SG
Potential complications of Nephrotic syndrome • Hypovolemic shock due to decrease intravascular volume. • Hypercoagulability (loss of protein result in the loss of coagulation proteins) can cause thrombi formation. • Respiratory compromise (due to fluid retention and abdominal distension. • Skin breakdown from massive edema • Infection (cellulitis, peritonitis, pneumonia, sepsis)
Laboratory evaluation UA • Proteinuria • Hematuria Blood tests • Decreased albumin level • Increased cholesterol level • Increased triglyceride level • Increased Hgb & Hct • Increased platelet count (can be as high as 500,000- 1 million)
Medical Management • Corticosteroid use: Prednisone or prednisolone to induce remission. 2mg/kg/d, response is usually within 7-21 days, dose will be tapered after 4-8 weeks. • Management of electrolyte imbalance • Protein replacement (either dietary or IV 5% albumin) . • Reduction of edema • Diuretic therapy must be used with caution to prevent intravascular depletion, thrombus formation and electrolyte imbalances • Dietary restriction of Na • Pain management • Prophylactic antibiotic therapy to prevent secondary infections caused by immunosuppression.
Medical Management Nephritis can be either acute or chronic. 2/3 of children will have a relapse. The chronic disease process is characterized by long term remissions and exacerbation, about 80% of children will eventually recover completely. For those children in who steroids fail to produce remission, they will be treated with immunosuppressant therapy, relapses are treated with high dose steroids
Nursing Interventions – Nephrotic Syndrome • Assess for respiratory distress :pulmonary edema • Assess for signs of hypokalemia: (arrhythmias, flat T waves, wide QRS, increased PR interval, decreased HR, hypotension. • Assess for signs of decreased cardiac function : hypotension, hypertension, CHF. • Assess for signs of hypo/hyponatremia due to diuretic use: Hyponatremia: • CNS: lethargy, weakness, apathy, dizziness, seizures, encephalopathy. • CV: hypotension Hypernatremia: • CNS: disorientation, muscle twitching.
Nursing Interventions – Nephrotic Syndrome • Assess for signs of infection: fever, cellulitis (from skin breakdown), peritonitis (red, tender abdomen), increased WBC • Assess for pain and comfort level • Parental and patient support • Daily weights, strict I & O • Activity is not restricted unless edema is extensive, ambulation should be encouraged • Diet: low salt during period of generalized edema, fluid restriction if edema is massive.
Wilm’s Tumor (Nephroblastoma) A intrarenal tumor. It is the most common malignant abdominal tumor of childhood. The tumor is separated from the kidney by a membranous capsule. It is a rapidly developing tumor. This capsule encloses the tumor, palpation of the tumor can cause the capsule to rupture disseminating cancer cells.
Wilm’s Tumor Prognosis for long term survival depends on stage at time of diagnosis, tumor cell markings and presence of metastasis (lungs, liver, other kidney). Over 75% of children have a 5 year survival rate. Most frequently seen between the age of 2-5 years, peak incidence at 3-4 years, rarely seen after the age of 7. There is a slightly higher incidence in boys. A small portion of Wilm’s tumors show a genetic basis. Almost exclusively unilateral, however can be bilateral : this is a very poor prognostic indicator.
Laboratory Tests/ Diagnostic criteria for Wilm’s tumor • Abdominal x ray • Ultrasound • CT • MRI • IVP
Clinical manifestation • Usually asymptomatic in early stages • Almost exclusively diagnosed after history from the mother/ guardian noting a mass while bathing the child located to one side of the abdomen. • Pain and hematuria may be present in some children. • Hypertension may be present (25%) due to increase in renin production.
Sign over bed “No abdominal palpation”. • Allergy alert bracelet & sign on chart, cardex stating “No abdominal palpation”.
Treatment • Nephrectomy to remove tumor and kidney, usually is done within 24-48 hours after diagnosis. • Follow up with chemotherapy for all children. • Bone marrow aspiration to rule out metastasis. • If bilateral, a partial Nephrectomy may be done to the least affected side .