Download

1 / 0
Clindamycin uses and concerns
0 likes | 202 Vues
Clindamycin uses and concerns. Dr.T.V.Rao MD. Clindamycin.
Télécharger la présentation 
Clindamycin uses and concerns
An Image/Link below is provided (as is) to download presentation
Download Policy: Content on the Website is provided to you AS IS for your information and personal use and may not be sold / licensed / shared on other websites without getting consent from its author.
Content is provided to you AS IS for your information and personal use only.
Download presentation by click this link.
While downloading, if for some reason you are not able to download a presentation, the publisher may have deleted the file from their server.
During download, if you can't get a presentation, the file might be deleted by the publisher.
E N D
Presentation Transcript
-
Clindamycinuses and concerns
Dr.T.V.Rao MD Dr.T.V.Rao MD - Clindamycin Clindamycin rINN is a Lincosamides antibiotic. It is usually used to treat infections with anaerobic bacteria but can also be used to treat some protozoal diseases, such as malaria. It is a common topical treatment for acne and can be useful against some methicillin-resistant Staphylococcus aureus (MRSA) infections. Dr.T.V.Rao MD
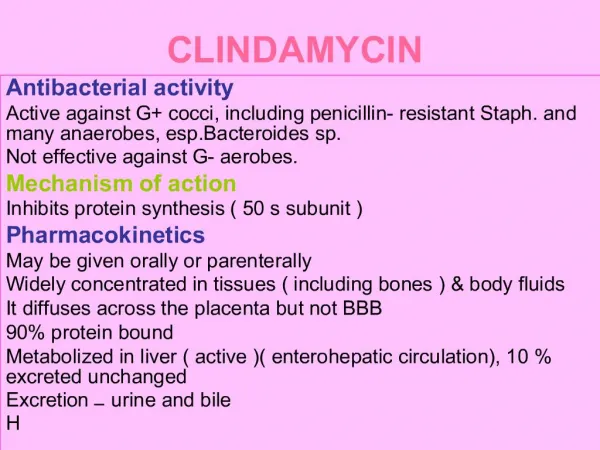
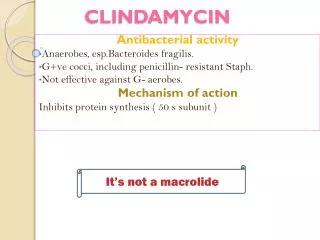
- Antibacterial activity Active against G+ cocci,including penicillin- resistant Staph. and many anaerobes, esp. Bacteroides sp. Not effective against G-ve aerobes. Dr.T.V.Rao MD
- CLINDAMYCIN Inhibits protein synthesis ( 50 s subunit ) Pharmacokinetics May be given orally or parenterally Widely concentrated in tissues ( including bones ) & body fluids It diffuses across the placenta but not BBB 90% protein bound Metabolized in liver ( active )( enter hepatic circulation), 10 % excreted unchanged Excretion – urine and bile Dr.T.V.Rao MD
- Clinical uses Staphylcoccal joint & bone infections such as osteomyelitis Staph. Conjunctivitis ( eye drops ) Diabetic foot infections Acne ( 1% topical gel & lotion ) Use Limited because of pseudomembranous colitis- can be fatal Dr.T.V.Rao MD
- Dr.T.V.Rao MD
- Testing for antibiotic resistance in clindamycin's differs from other bacteria The detection of its three resistance phenotypes (sensitive, resistant, inducible resistance) is crucial to guide antimicrobial therapy. Standard disk diffusion and broth micro dilution fail to detect inducible clindamycin resistance . Clinical and Laboratory Standards Institute (CLSI) recommends the double disk diffusion test (D-test) to detect the presence of inducible clindamycin resistance . Also, the incidence of clindamycin resistance varies with geographic area and therefore local statistics are crucial to guide empiric therapy Dr.T.V.Rao MD
- clindamycin-erythromycin discordant Clindamycin-susceptible, erythromycin-resistant Staphylococcus aureus (clindamycin-erythromycin discordant) may develop clindamycin resistance. The erm gene product is a ribosome methylase whose expression is normally minimal. Erythromycin induces the production of this methylase, which is why these strains are erythromycin resistant, but mutations in the promoter region of erm allow production of methylase without an inducer Dr.T.V.Rao MD
- Testing for erythromycin and clindamycin resistance is a priority Dr.T.V.Rao MD
- The D-test for Macrolide-Inducible Resistance to Clindamycin A positive D test indicates the presence of macrolide-inducible resistance to clindamycin produced by an inducible methylase that alters the common ribosomal binding site for macrolides, clindamycin and the group B Streptogramins (Quinpristin)(Woods, 2009) . The cross-resistance, called the MLS-B phenotype, results from enzymatic methylation of an adenine residue of the 23S component of the 50S ribosomal subunit that these 3 drug groups bind to. The methylase is encoded by a plasmid-borne gene erm. This genotype has been associated with clinical reports of clindamycin failure. As a result the “Clinical and Laboratory Standards Institute” (a nonprofit standards organization) recommends that laboratories report D-test+ isolates as “resistant to clindamycin” (NCCLS 2004; Woods, 2009). Dr.T.V.Rao MD
- D test will identify the inducible resistance These mutants are stably erythromycin and clindamycin resistant. Since erythromycin resistance can occur with other mechanisms. (e.g., efflux pumps and enzymatic modification) the D-test identifies inducible resistance that might presage mutational clindamycin constitutive resistance. Dr.T.V.Rao MD
- A negative D- Test A negative D-test observed for an erythromycin-resistant culture of S. aureus. The small discs labeled E & C represent disks containing either 15 μg erythromycin (E) or 2 μg clindamycin (C) placed 15 to 20 mm apart on an agar plate that has been inoculated with the clinical isolate (indicated by the green background). The lack of a zone of inhibition around the erythromycin disc indicates bacterial resistance to macrolides The large clear zone of inhibition around the clindamycin disc indicates sensitivity to clindamycin Dr.T.V.Rao MD
- A positive d- test A positive D-test. Diffusion of erythromycin from the disc towards the clindamycin disc does not kill bacteria due to S. aureus resistance to macrolides. However, in this case the bacterial isolate contains a strain of S. aureus with an erythromycin-inducible methylase (iMLS-B) resulting in inhibited growth. The inhibition of bacterial growth in zone 2 but not zone 1 produces a “D” shape surrounding the clindamycin disk, which is considered a “positive” D-test. (Adapted from Woods 2009). Dr.T.V.Rao MD
- Performing D- Test The D-test is performed by placing clindamycin and erythromycin disks at an edge-to-edge distance of 15 to 20 mm and looking for flattening of the clindamycin zone nearest the erythromycin disk . A positive D-test suggests the presence of an erm gene that could result in constitutive clindamycin resistance and clinical failure. Dr.T.V.Rao MD
- When to avoid use of clindamycin Clindamycin may still be effective in some patients with this phenotype, the working assumption is that the isolate is “presumed” to be resistant based upon detection of inducible clindamycin resistance. For serious infections such as sepsis, pneumonia, or other invasive S. aureus infections, even the small risk of emergence of resistance to clindamycin as indicated by a positive D-test should lead to avoidance of use of clindamycin(Woods, 2009). Dr.T.V.Rao MD
- Clindamycin in malaria Given with chloroquine or quinine, clindamycin is effective and well-tolerated in treating Plasmodium falciparum malaria; the latter combination is particularly useful for children, and is the treatment of choice for pregnant women who become infected in areas where resistance to chloroquine is common. Clindamycin should not be used as an antimalarial by itself, although it appears to be very effective as such, because of its slow action. Patient-derived isolates of Plasmodium falciparum from the Peruvian Amazon have been reported to be resistant to clindamycin as evidenced by in vitro drug susceptibility testing.[ Dr.T.V.Rao MD
- Adverse complications with clindamycin Common adverse drug reactions (ADRs) associated with clindamycin therapy — found in over 1% of patients — include: diarrhea, pseudomembranous colitis, nausea, vomiting, abdominal pain or cramps, rash, and/or itch. High doses (both intravenous and oral) may cause a metallic taste, and topical application may cause contact dermatitis.Diarrhea, vomiting, and nausea are common if the individual lies down for an extended period of time within 30 minutes of taking clindamycin. In addition, severe heartburn can be expected for up to three days if the individual does not stay in an elevated position for at least 30 minutes. Dr.T.V.Rao MD
- Colitis is a feared complication Clindamycin has been associated with colitis (inflammation of the bowel); this is caused by a toxin produced from an overgrowth of a bacterium, Clostridium difficile. Symptoms can range from mild watery Diarrhoea to severe, persistent Diarrhoea with fever, abdominal cramps and the passage of blood and mucus. It may be potentially serious. If significant Diarrhoea develops whilst taking clindamycin, the drug should be stopped. A stool test may show the presence of the toxin. Dr.T.V.Rao MD
- Pseudomembranous colitis is a potentially lethal condition Pseudomembranous colitis is a potentially lethal condition commonly associated with clindamycin, but which occurs with other antibiotics, as well. Overgrowth of Clostridium difficile, which is inherently resistant to clindamycin, results in the production of a toxin that causes a range of adverse effects, from diarrhea to colitis and toxic mega colon. Rarely — in less than 0.1% of patients — clindamycin therapy has been associated with anaphylaxis, blood dyscrasias, polyarthritis, jaundice, raised liver enzyme levels, and/or hepatotoxicity. Dr.T.V.Rao MD
- Precautions in use of clindamycin The safety of use in pregnancy has not been established. Clindamycin has been reported to appear in breast milk. If therapy is prolonged, liver and renal function tests may be monitored periodically. May enhance the action of neuromuscular blocking agents. May counteract the effects of erythromycin Dr.T.V.Rao MD
- Programme created by Dr.T.V.Rao MD for Medical and Health Care workers in the Developing world Email doctortvrao@gmail.com Dr.T.V.Rao MD




More Related