Download

1 / 1
10 likes | 103 Vues
Investigating genetic alterations in VHL and p53 genes in RCC, correlating with tumor behavior. Methods include PCR-SSCP sequencing and immunohistochemistry. Results show somatic VHL mutations impacting tumor progression.

E N D
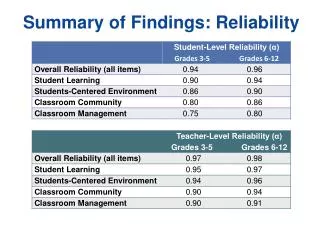
Abstract #520 (P31) SOMATIC VHL BUT NOT P53 MUTATION IN SPORADIC CLEAR CELL RENAL CELL CARCINOMASMeye A1,2*, Taubert H2, Hinze R2, Bilkenroth U2, Göhring B1,3, Rebmann U4, Riemann D3, Heynemann H11 Clinic of Urology, 2 Institute of Pathology, and 3 Institute of Medical Immunology, University Halle, and 4 Department of Urology, Diakonissenanstalt Dessau, Germany[ *present email: axel.meye@mailbox.tu-dresden.de / web: http://www.medizin.uni-halle.de:81/molekularpathologie/]A.M. was supported by a grant from the “Novartis Stiftung für Therapeutische Forschung e.V.” (Germany). SUMMARY INTRODUCTION & OBJECTIVES: For patients suffering from renal cell carcinomas (RCC) a variability in the clinical course is known. The potential role of genetic alterations in tumor suppressors is not investigated comprehensively. The identification of multiple or/and combined genetic alterations may give the opportunity to correlate those results with the expected biological behaviour of an individual tumor. MATERIAL & METHODS: We established a RCC bank with clinical and immunohistochemical data and isolated genomic DNA. To evaluate the molecular genetic status in the tumor suppressors genes VHL and p53 in RCC, a non-radioactive PCR-SSCP-sequencing strategy using genomic DNA from 38 cases and three RCC cell lines was applied. Tumor and renal parenchymal normal tissue samples were also investigated by immunohistochemistry for both antigens and for proliferation index (Mib-1) and apoptosis rate (TUNEL-assay). Furthermore, we evaluated the VHL and p53 protein expression also by Western blot hybridisation. RESULTS: In contrast to the p53 gene (exons 4-9), were no gene alteration was found, in five cases mutations (four clear-cell tumor samples and one cell line) in the VHL coding region could be identified, resulting in four cases to a internal early stop codon. AlI four mutations identified in vivo had a somatic origin as further investigation of the corresponding kidney parenchymal tissue could shown. All four tumors were characterised by a relativ high proliferation and two cases had a increasd apoptotic index in comparison with the non-mutated RCC samples studied. Interestingly, for two patients with somatic VHL mutations an increased tumor frequency of carcinomas were determined in a retrospective study: One sister of one patient had had also a aggressive RCC in the same age. Generally, we found a distinct reduced pVHL expression level determined by IHC and western blot. In Western blot analyses generally a decrease for VHL expression compared to the parenchym could be confirmed. CONCLUSIONS: Taken together, we found a distinct role of VHL frameshift mutations but not of p53 for non-familial RCC and a good correlation of IHC and Western blot analysis in determination of the mutational effects on the protein level. The finding of a intrafamiliar coincidence of RCCs with a somatic VHL mutation and need further evaluations. Material & Methods Tumor material and patients Fresh tumor and corresponding normal kidney tissues were obtained from patients undergoing nephrectomy for renal cancer in the time period 1994-1997 at the University Halle-Wittenberg. All patients (n= 38) were treated at the same clinical centre (Urological Clinic, Univertsity Halle) independently from the molecularly studies and findings. Altogether, 38 primary RCC from 25 males and 13 females (medium age at the date of nephrectomy: 57 years with a range of 36 to 73 years) and with an median follow-up of zz months were investigated. The diagnosis was established by histopathological examination (hematoxylin and eosin staining) according the Thoenes et al. classification. Altogether, 19 clear cell, 7 clear cell/chromophilic, and both six chromophilic and six chromophobe tumors were investigated.Briefly, a grossly non-necrotic tumor area was divided in two parts; the fresh material was fixed in buffered formaldehyd and embedded in paraffin (histological investigations) or snap-frozen in liquid nitrogen and stored at –80°C (molecular studies). Furthermore, corresponding normal parenchymal tissue was available of the kidney. For immunhistochemistry, paraffin embedded tumor samples from 24 of the 38 patients (17 males, 7 females) with a medium age of 57 years (36-73) were investigated. Immunohistochemistry (IHC) A p53-overexpression was determined using the monoclonal Do-7 antibody (dilution 1:200; Oncogene Science, Hamburg, Germany) whereas the pVHL expression was studied by the monoclonal anti-VHL antibody (65031A, dilution 1:50; Pharmingen, Hamburg, Germany). For immunhistochemically detection of P53 and VHL protein expression exclusively paraffine-embedded sections (4-6 µm) were processed after antigen retriveal with microwave. The detection system used was based on the ABC system (Dako, Hamburg, Germany). Stained sections were assessed by two different investigators without knowledge of the clinical or histological diagnosis. IHC staining pattern were evaluated by light microscopy semi-quantitatively for staining intensity and proportion of tumor cells labeled into for stages (strong, medium, weak, negative) according to a schema described previously (Göhring et al. 1998). Furthermore, the VHL and p53 staining pattern of the tumor cells was compared to adjacent normal epithelium (as an internal standard expression level). Western Blot Total protein was extracted from frozen tumor sections using standard procedures and the protein concentration was carried out (protein concentration assay, Sigma). Equivalent amounts of total protein (30 µg) was separated electrophoretically in polyacrylamide gels (10 or 12.5 %), blotted on PVDF membrane (0.5 µm pore size; Millipore) and were incubated with the primary (pVHL dilution 1:100, p53 Do-7, 1:100, bcl-2 Ab-1, 1:50, Calbiochem) and a secondary antibody (anti-rabbit P0448, dilution 1:2000, anti-mouse P0260, dilution 1:1000, Dako) both for one hour. The antigen-antibody reaction was detected by chemiluminiscence (ECL system, Amersham, Braunschweig, Germany) on X-ray films (BiomaxTM, Kodak, Braunschweig). As an additional internal control for equivalent total protein amounts a control hybridisation with a –actin antibody (AC-40, dilution 1:1000, Sigma) was carried out. Mutational analysis Genomic DNA from frozen tumor sections (60 µm) was isolated according to standard methods (Taubert et al. 1995). Polymerase chain reactions (PCR) for the p53 gene (Exons 4-9, five PCR fragments), the VHL gene (Exons 1-3, 4 PCR fragments) performed as described in Table 2. For each amplification strategy (100 ng genomic DNA) in a thermocycler (TrioblockTM Biometra, Göttingen, Germany) following PCR conditions were used: 5 min at 92°C; 35 or 40 cycles of at annealing temperature for 30, 45 or 60 s (Table 2), 1 min at 72°C ; and a final extension step of 72°C for 5 min. Equivalent amounts of PCR products were prescreened in a non-radioactive single-strand conformational polymorphism (SSCP) analysis (Würl et al. 1996). Briefly, 6-12 µl were separated in 6 or 10% ready-made polyacrylamide gels containing 2-3% glycerol (TBE-gels; Novex, Heidelberg, Germany) for 2-3 hours at 90 V. Afterwards, the DNA bands were visualized by a standard silver staining method (Promega). Samples with shifts in the single strand DNA pattern, indicating a mutation, were purified (Qiagen PCR Purification Kit, Qiagen, Hilden) and cycle-sequenced (with SE & AS PCR primer) using the Dye Amplitaq Terminator FS strategy and an ABI373 (Perkin Elmer, Weiterstadt, Germany). All sequence alterations were confirmed by at least two independent PCR-SSCP-sequencing experiments before calling mutational events. ssDNA ssDNA 39-96 Fig. 3 Fig. 4 dsDNA Fig. 1: Representative SSCP results for the PCR fragment 1b of the VHL gene. In the case of 39/96 an abnormal band shift is shown, the adjacent direct sequencing produce an eight base pair frameshift (Table) • SUMMARY OF KEY FINDINGS • VHL and p53 mutational analysis • In the SSCP-analyses only for four different p53 PCR-fragments a weak band shift was identified. However, we found no gene alteration in exons 4 to 9 of the p53 TSG in multiple independent sequencing reactions. In contrast, for 11 samples (5 cases for overlapping fragments) a SSCP shift for the VHL gene were identified (Fig. 1). In the following sequencing altogether five VHL mutations (four in exon 1 and one for exon 2) in four of the 38 RCC samples (11%) and in the cell line Caki-1 (codon 69) were determined (Table). To exclude a germline origin of the identified VHL gene alterations in vivo, we screened additionally the corresponding parenchymal tissue of the affected kidneys by direct sequencing. But we could not confirm the mutation in the corresponding parenchymal tissue sample indicating a somatic event for all mutations found in vivo. These four mutations were found exclusively in clear cell tumors, although one showed additionally chromophilic proportion. All four tumors were characterised by a relativ high proliferation in comparison with the non-mutated RCC samples (15 %) studied. The mutation of the case 09/96 was found for a patient of a family with further tumor cases, who had a primary metastatic process. He died three months after the nephrectomy. The other three patients with VHL-mutated RCC had a median follow-up of 33 months. Interestingly, for one patient we found by reevaluation of the clinical data a familial cancer connection. The patient had a carcinoma of the colon shortly before the RCC was diagnosed. In the mean time he got metastasis in the liver (Table). The sister had also a RCC in one kidney three years before him. Up to now (more than five years after nephrectomy) she is without relapse. Interestingly, for one further tumor sample (RCC39/96) additionally a carcinoma in situ for the same tissue could be evaluated. However, because of the relative short follow-up of the affected patients we can not state a prognostic value of the somatic VHL mutations but we found a increased incidence of histological and familial characteristics supporting a biological role of the gene alterations in the genesis of these RCCs. Moreover and in contrast to the literature, a missense mutation in the codon 69 was identified for the cell line Caki-1 (Knebelman et al. 1998). • Immunohistochemistry (p53, VHL, Ki-67, TUNEL) • In 6 out of 24 the samples (25%) the p53 gene product was detected indicating a protein-overexpression (data not shown). No correlation of p53 positivity to the grading was found (each 3 cases for grade 2 and grade 3 tumors). In normal kidney parenchymal samples a strong cytoplasmatic staining for the VHL gene product was identified. In contrast, all investigated RCC tissues showed a strong decrease in the VHL expression. Fourteen tumor samples (58%) had lost completely the expression (<1% positive tumor cells), whereas 7 cases (29%) had low (5-20% positive) and only 3 cases (13%) moderat conservation (20-50% positive) of the VHL expression pattern. There was a tendency of a higher VHL expression level in RCCs of the clear cell type, because 12/14 of these tumors (86%) had detectable VHL protein (>5% positivity). In contrast to the VHL mutated cases only a minority of RCCs without a VHL mutation showed high proliferation activity (two cases with >20% Ki-67 positive tumor cells) (Table). All non-muted were characterized by a low apoptotic index with a maximum of 5% TUNEL-positive cells. • Western blot results (p53, VHL, Bcl-2) • With Western blot analysis we could confirm the observations of immunohistochemistry for both tumorsuppressors. Normal cells originating from the kidney containing the RCCs expressed no or a low p53 protein level. But in many cases with a strong decrease of VHL expression in the tumor we detected simultaneously an induction of p53 activity (Fig. 2). Furthermore, a relative high Bcl-2 expression in both tumor and parenchym support the relative low apoptotic rates determined by the TUNEL assay. The Bcl2-expression rate was independent from the VHL gene status (Fig. 3). Table: Identified intragenic VHL mutations, histological and clinical data of the affected RCC patients Abbreviations: a-alive, aa-amino acid, alt-alteration, bp-base pairs, c-clear cell type, cp- chromophile type, cod-codon, d-dead, del-deletion, f-female, fa- familial anamnese, fs-frameshift, hist-histology, m-month(s), M-detection of metastases at the time of diagnosis, mut-mutation, N-lymph node status, nd-not determined, sv- survival time after nephrectomy in months, trunc-truncation, T- Tumor size The identified fs in sample 9-96 results in a new stop at nt 685. For the patient 9-96 a metastatic process was evaluated at the time of nephrectomy. Additionally, the grant mother of the patient had a carcinoma of the liver. For the affected patient 24-96 one month before the nephrectomy a colon carcinoma was diagnosed and resected. Additionally, the sister had also a nephrectomy because of a RCC four years before him (in 1992). In the meantime a metastatic process was diagnosed (04/98, in the liver, G3 adenocarcinoma), propably originated from the colon carcinoma. For patient 39-96 a carcinoma in situ in the same tumor tissue sample were identified (dysplasie 2-3). 04-96 05-96 17-96 04-97 01-96 02-96 RD P T P T P T - P T P T P T - C P53 pVHL ß-actin ? tumor alteration 35-94 09-96 24-96 39-96 RCCs with mt-VHL miss fs fs fs mutation type P T P T P T - P T Bcl-2 ß-actin Fig. 2 & 3: Western blot results for p53, VHL and Bcl-2 proteins in tumor and parenchymal samples from RCCs