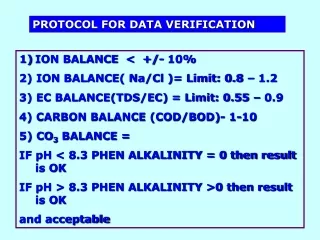
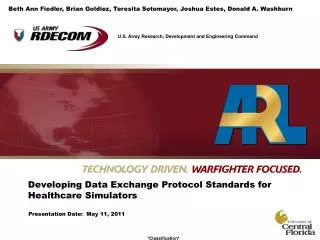
Developing Data Exchange Protocol Standards for Healthcare Simulators
Beth Ann Fiedler, Brian Goldiez, Teresita Sotomayor, Joshua Estes, Donald A. Washburn. Developing Data Exchange Protocol Standards for Healthcare Simulators . Presentation Date: May 11, 2011. Outline. Introduction Purpose IEEE1278 Standard

Developing Data Exchange Protocol Standards for Healthcare Simulators
E N D
Presentation Transcript
Beth Ann Fiedler, Brian Goldiez, Teresita Sotomayor, Joshua Estes, Donald A. Washburn Developing Data Exchange Protocol Standards for Healthcare Simulators Presentation Date: May 11, 2011
Outline • Introduction • Purpose • IEEE1278 Standard • Facilitating Interoperability and Standards for Simulators in Healthcare • Key Elements of Patient Information and Medical Systems • The Role of the Injury Severity Score • Missing Parameters and Source for Medical Simulator Information • Medical Coding Systems • Data Set Coding Structures • DICOM • Conclusion • References
Introduction • MedBiquitous, a nonprofit organization founded by Johns Hopkins Medicine, has developed a Virtual Patient (VP), ANSI VP.10.1-2010 • The US Army is interested in prototyping a structure to exchange physiological information between simulators • Leveraging existing standards and programs • Consistent and growth with existing simulators • Useful by non-DoD entities • This structure is currently being considered by the SISO for IEEE balloting • Creation of system architecture for translation of clinical conditions to Virtual Patient • IEEE1278 Protocol Data Units • DICOM Hierarchical Client-Server System Architecture • Current medical coding system (e.g., ICD-9, ICD-10, SNOMED-CT, DRG, and CPT) • Medical history • Integrated and human readable virtual patient chart • In situ simulation → point of injury data access
Purpose • Goal: Create an interoperability standard amongst computer based medical simulators and between medical & other simulated entities • Benefit: Potential to increase the functionality, utility, training effectiveness, and realism needed to properly train and maintain proficiency among medical professionals in both the private and government sectors • Opportunity: Create standard interchange protocols.
IEEE 1278 Distributed Interoperable Simulation (DIS) • IEEE 1278 Distributed Interactive Simulation (DIS) • Interchange between virtual simulators communities since 1995 • Utilizes Protocol Data Units (PDUs) • Multiple connection strategies, real time, no central clock, uses a heart beat, dead reckoning, etc. • Built from DARPA SIMNET Program • Contains Entity State PDU (which includes life forms) • Opportunity for Enhanced Medical Relevance • DICOM PDUs • Medical Code PDUs • Simulation Interoperability Standards Organization (SISO) manages and ballots changes for the IEEE • Compatible with Army’s Program Executive Officer – Simulation, Training and Instrumentation (PEO-STRI) • Leverages Synthetic Environment Core (SE CORE)
Facilitating Interoperability and Standards for Simulators in Healthcare • Protocol Data Units (PDUs) • Data messages passed between network simulation applications • IEEE Standard 1278.1, Draft 15 contains 60 PDU instances • Proposed Virtual Patient information and data • Leverages Medbiquitous Virtual Patient • Entity State PDU: low fidelity data about VP using Variable Parameter • Attribute PDU: higher fidelity info about VP via its Attribute Records • Entity State PDU • Defines all entities in the simulated environment (e.g., Life Form PDU) • Basic Patient Data • Physiological Data • Current design use cases • Transfer ownership • Supply consumables • Partial control of parameters
Facilitating Interoperability and Standards for Simulators in Healthcare • Variable Parameter • Used by Entity State PDU to store basic information • 128 bits in length, holds pertinent virtual patient information • Lower-fidelity information • Attribute Record • Similar to Variable Parameter records with exceptions • Attribute Records are not part of an Entity State PDU • Attribute Records have no bit limitations (infinite storage capacity) • Attribute Records are useful for high fidelity patient data
Facilitating Interoperability and Standards for Simulators in Healthcare Figure 3: The Extended Lifeform Basic Attributes Variable Parameter record. This data structure is used to hold lower-fidelity virtual patient data inside of an Entity State PDU. Figure 1: The 11 physiological systems as represented by Attribute Records (IEEE 1278). These records hold higher-fidelity virtual patient data. Figure 2: A closer look at the Cardiovascular System Attribute Record. Note that the parameters are separated into 64-bit blocks. Figure 4: A diagram outlining one possible method for “sharing ownership” of a virtual patient. The main steps include: 1)Creating and copying a patient (so that one exists in each application) and 2) Querying and setting patient information so that both patients’ statuses are the same.
Our Focus: Conveying Additional Relevant Information • Significant gap in translating clinical conditions to the Virtual Patient (VP) • Existing healthcare medical coding systems may provide the basis to demonstrate dynamic patient episodes of care through the expression of physiological conditions supporting the current state of the VP • Clinical conditions and other patient data from actual/simulated from medical service encounters incorporated into medical simulation training • Triage • Physician office visits • Hospital emergency • Surgical procedures • Current Proposition • Medical codes can be reverse engineered to create a virtual chart • Specific patient • A class of patients • Access to images can augment codes • Data can be packaged into PDUs.
Medical Coding Systems • International Classification of Diseases, Clinical Modification,9th Revision (ICD-9-CM) • US payer system developed by AHA, AHIMA, NCHS • Three to five digit field length with variations • External Cause of Injury (E) • Reason for Encounter (V) • Morphology (M) • 13,000 codes in ICD-9-CM Diagnosis Volumes 1 and 2 • 3,000 codes in ICD-9-CM Procedure Coding System Volume 3 • Classification expansion prohibited due to data structure
Medical Coding Systems • International Classification of Diseases, Clinical Modifications, 10th Revision (ICD-10-CM/PCS) • Consists of Clinical Modification (CM) and Procedures Coding System (PCS) • Dominant payer system outside US, expandable • Three to seven alphanumeric digits • External Cause of Injury (ICD-9 E Codes) embedded in new structure • Reason for Encounter (Z) from ICD-9 V Codes • Morphologies (C, D) • CMS projected change October 2013 developed in US by AHA, AHIMA, CDC, CMS • 68,000 codes ICD-10-CM consolidates ICD-9 V1 and V2 • 72,000 codes ICD-10-PCS replaces ICD-9 V3
Medical Coding Systems • Systemized Nomenclature of Medicine, Clinical Terms (SNOMED-CT) • Provider system developed by CAP to capture primary diagnosis • Four to nine digit numeric codes, first character alphanumeric • 366,170 Terminologies • One million English language descriptions • 1.46 million semantic relationships • Current Procedural Terminology (CPT) • Payer system for non-hospital physician services developed by AMA • Five digit standard, first character alphanumeric • Symbol and numeric modifiers to reduce payment time • 7800 codes • Diagnostic Related Groups (DRG) • Internal facility system determines resource utilization developed by CMS • 500 Medical/Surgical Groups, 1,200 Subclasses • Medicaid Severity MS DRG common three to five digit codes*
Enhanced Medical PDU Designedto support conveyance of data between disparate systems Not the manipulation at either end point
Data Set Coding Structures Proposed MEDICAL CODING SET PDU (Partial)
Digital Images and Communication in Medicine (DICOM) • ISO-OSI model of communication • Established by ACR and NEMA in 1982 • Initial use: transfer of radiology data, data storage • Current use: Network Protocol Digital Archive and Communication System • Non radiology expansion • 20 Working Groups (e.g., nuclear medicine, cardiology) • International Acceptance • Opportunity to optimize DICOM protocols • Establish workflow • Create unique VP data exchange identifiers • Permit computer-based mannequins or simulator communication • Permit communication between clinical equipment modalities and VP • Magnetic Resonance Imaging (MRI) • Computed Topography (CT) • Ultrasounds (US)
Digital Images and Communication in Medicine (DICOM) Proposed DICOM PDU
Digital Images and Communication in Medicine (DICOM) Figure 5. Proposed Protocol Data Units for Digital Images and Communication in Medicine (DICOM) Element Indicating Image Hierarchy
Status and Plans • Feedback being sought • Healthcare user community • Manufacturers • Regulators/Decision Makers • Basic Life Form PDU being prepared for IEEE review & balloting • Presented at IMSH (Jan ‘11) • Presented at SIW (Apr ‘11) • Attribute PDU for physiology being prepared for IEEE review & balloting • Presented at IMSH (Jan ‘11) • Presented at SIW (Apr ‘11) • Prototyping underway with data converters • General physiology model • Simulator manufacturer’s model • Coding and DICOM being prepared for IEEE review & balloting • Tutorial for I/ITSEC being prepared for review
Conclusions • Short Term Benefits • Increased VP Capabilities • Transmit entity information • Transfer an entity between multiple simulation applications • Approximate impact on entity’s in proximity to a simulated explosion • Flexible roadmap to incorporate medical coding systems that expand the interoperability standards in healthcare simulation • Restores capture of most condition information • Potential to overcome inability to capture all written, verbal, and interpretive information not presently translated in billing/payment driven medical coding systems • Long Term Benefits • Overcomes present inability to view dynamic body changes in patient injured condition • Growth as simulators grow • Recognized standard body for developers, users, managers
References Advanced Technology Applications for Combat Casualty Care (ATACCC). Proceedings of the ATACCC Conference August 16-19, 2010. St. Pete Beach, FL. Alexander, S., Conner, T., & Slaughter, T. (2003). Overview of inpatient coding. American Journal of Health-System Pharmacy, 60(21 Suppl 6): S11-4. Cardillo, E., Eccher, C., Serafini, L. &Tamilin, A. (2008). Proceeding AIMSA '08 Proceedings of the 13th international conference on Artificial Intelligence: Methodology, Systems, and Applications Springer-Verlag Berlin, Heidelberg. doi>10.1007/978-3-540-85776-1_26 . Centers for Medicare & Medicaid Services, Department of Health and Human Services. Medicare program; hospital inpatient prospective payment systems and FY 2005 rates. Final rule. Federal Register 69, no. 154 2004a (August 11); 48916–49781. Institute of Electrical and Electronics Engineers, Inc. IEEE Standard P1278.1/D15. (2010, April). IEEE Draft Standard for Distributed Interactive Simulation—Application Protocols. Pianykh, O. S. (2008). Digital Imaging and Communications in Medicine (DICOM): a Practical Introduction and Survival Guide. Berlin: Springer.
The Role of the Injury Severity Score (ISS) • ISS Primary role Pre-Treatment • Triage • Chief Complaint • Review of Systems • Comparable Acute Care Case Mix Complexity • Assessment Post Treatment Historical Analysis • Resource utilization
Key Elements of Patient Information and Medical Service • Creation of a virtual chart • PDU Data Source: 4 patient data elements • Chief Complaint • Review of Systems (body) • History of Present Illness • Medical History • 1 & 2 focus of current efforts • 3 & 4 verbal or scripted (technological gap in IEEE 1278)
Digital Images and Communication in Medicine (DICOM) http://www.mfdigital.com/images/dicom.jpg