Download
1 / 4
70 likes | 222 Vues
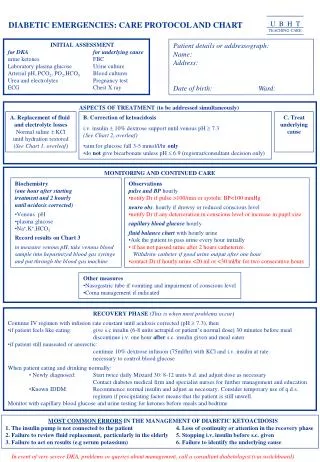
U B H T TEACHING CARE. DIABETIC EMERGENCIES: CARE PROTOCOL AND CHART. INITIAL ASSESSMENT for DKA for underlying cause urine ketones FBC Laboratory plasma glucose Urine culture Arterial pH, PCO 2 , PO 2 ,HCO 3 Blood cultures Urea and electrolytes Pregnancy test ECG Chest X ray.

E N D
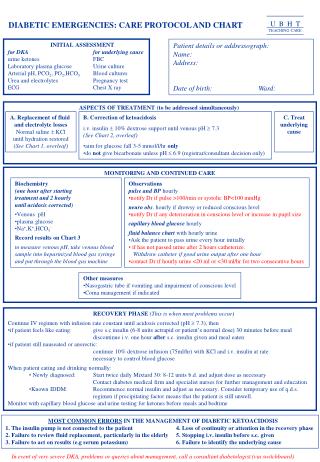
U B H T TEACHING CARE DIABETIC EMERGENCIES: CARE PROTOCOL AND CHART INITIAL ASSESSMENT for DKA for underlying cause urine ketones FBC Laboratory plasma glucose Urine culture Arterial pH, PCO2, PO2,HCO3 Blood cultures Urea and electrolytes Pregnancy test ECG Chest X ray Patient details or addressograph: Name: Address: Date of birth: Ward: ASPECTS OF TREATMENT (to be addressed simultaneously) A. Replacement of fluid and electrolyte losses Normal saline KCl until hydration restored (See Chart 1, overleaf) • B. Correction of ketoacidosis • i.v. insulin 10% dextrose support until venous pH 7.3 • (See Chart 2, overleaf) • aim for glucose fall 3-5 mmol/l/hr only • do not give bicarbonate unless pH 6.9 (registrar/consultant decision only) C. Treat underlying cause MONITORING AND CONTINUED CARE • Biochemistry • (one hour after starting • treatment and 2 hourly • until acidosis corrected) • Venous pH • plasma glucose • Na+,K+,HCO3- • Record results on Chart 3 • to measure venous pH, take venous blood sample into heparinized blood gas syringe and put through the blood gas machine • Observations • pulse and BP hourly • notify Dr if pulse >100/min or systolic BP<100 mmHg • neuro obs. hourly if drowsy or reduced conscious level • notify Dr if any deterioration in conscious level or increase in pupil size • capillary blood glucose hourly • fluid balance chartwith hourly urine • Ask the patient to pass urine every hour initially • if has not passed urine after 2 hours catheterize. • Withdraw catheter if good urine output after one hour • contact Dr if hourly urine <20 ml or <30 ml/hr for two consecutive hours • Other measures • Nasogastric tube if vomiting and impairment of conscious level • Coma management if indicated • RECOVERY PHASE (This is when most problems occur) • Continue IV regimen with infusion rate constant until acidosis corrected (pH 7.3), then • if patient feels like eating: give s.c insulin (6-8 units actrapid or patient’s normal dose) 30 minutes before meal • discontinue i.v. one hour after s.c. insulin given and meal eaten • if patient still nauseated or anorectic: • continue 10% dextrose infusion (75ml/hr) with KCl and i.v. insulin at rate • necessary to control blood glucose • When patient eating and drinking normally: • Newly diagnosed: Start twice daily Mixtard 30: 8-12 units b.d. and adjust dose as necessary • Contact diabetes medical firm and specialist nurses for further management and education • Known IDDM: Recommence normal insulin and adjust as necessary. Consider temporary use of q.d.s. regimen if precipitating factor means that the patient is still unwell. • Monitor with capillary blood glucose and urine testing for ketones before meals and bedtime MOST COMMON ERRORS IN THE MANAGEMENT OF DIABETIC KETOACIDOSIS 1. The insulin pump is not connected to the patient 4. Loss of continuity or attention in the recovery phase 2. Failure to review fluid replacement, particularly in the elderly 5. Stopping i.v. insulin before s.c. given 3. Failure to act on results (e.g serum potassium) 6. Failure to identify the underlying cause In event of very severe DKA, problems or queries about management, call a consultant diabetologist (via switchboard)
CHART 1: FLUID AND ELECTROLYTE REPLACEMENT USUAL ADULT REQUIREMENT • Normal saline (0.9%) - 1 litre in first 30 min - 1 litre in next hour -Review - Continue saline infusion until hydration restored (with simultaneous dextrose infusion if indicated) • Potassium <3.5 mmol/l: 40 mmol/l KCl 3.5-5.5 mmol/l: 20 mmol/l >5.5 mmol/l: Stop KCL STOP KCl IF THE PATIENT IS ANURIC (Aim to keep K+ in the range 4.0 - 5.5 mmol/l) Do not givebicarbonate unless pH 6.9. If necessary use 1.4% solution + 20 mmol KCL. Always discuss with Registrar or Consultant before giving HC03 . Refractory acidosis may result from inadequate fluid and electrolyte replacement. Page 2
Chart 2: CORRECTION OF KETOACIDOSIS: GLUCOSE AND INSULIN INFUSIONS If BG has risen since the last measurement, inspect pump, cannula and all connections - this problem is always caused by insulin not actually getting into the patient Contact Dr if • blood glucose falls more than 10 mmol/l in one hour • blood glucose has risen since the last measurement and the pump and all connections are intact Page 3
Chart 3: LABORATORY RESULTS Monitoring: One hour after starting treatment and 2 hourly until acidosis corrected • Venous pH • Laboratory plasma glucose • Na+, K+, HC03- Initial investigations: For DKA: For underlying cause: • Plasma glucose • FBC • Arterial blood gases •Urine culture • Urea, electrolytes, HCO3-• Blood cultures • ECG • Pregnancy test (urine HCG) • Chest X ray Contact Dr if: • Venous pH <7.30 and has not risen since last measurement • Plasma glucose falls by more than 10 mmol/l per hour, or if plasma glucose is above 15 mmol/l and has not fallen over 2 hours • Na+ <130 or > 155 mmol/l • K+ <3.5 or >5.5 mmol/l Page 4