Download
1 / 18
180 likes | 184 Vues
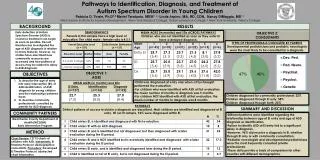
Pathway Granularity and solutions to Barriers to Sepsis diagnosis and treatment. Background. The management of the patient with sepsis in the first hour is a time critical emergency and requires a team based approach involving all relevant healthcare staff members. Responsibility

E N D
Pathway Granularity and solutions to Barriers to Sepsis diagnosis and treatment
Background The management of the patient with sepsis in the first hour is a time critical emergency and requires a team based approach involving all relevant healthcare staff members. Responsibility It is the responsibility of the multidisciplinary team to administer the elements of the Sepsis 6 within the recommended timeframe.
Aim Statement In November 2015 reviewing 8 patients on surgical ward who triggered for Sepsis the average wait time to be reviewed by a doctor was 53 minutes. Our aim is to reduce this time to less than 30 minutes by March 2015.
SEPSIS Goal* Patient should be reviewed by the Senior House Officer within 30 minutes of triggering with a score of 4-6. A score of over 6 - the patient is for an immediate review. *National Guidelines for Sepsis Management and in The National Early Warning Score Guidelines No. 1 Feb 2013 pg 75.
Driver Diagram Secondary Drivers Primary Drivers • Executive management board engagement. • Involve staff to embrace and grow a culture of Safety and Quality Improvement in relation to Sepsis. • Continuous Improvement through Clinical Leaderships/Governance and Champions working towards a shared goal. • Education of Multidisciplinary team. • Honest/transparent measurement of performance delivered monthly to EMB. Building a Patient Safety Culture Result : Mean wait time to review was 43.7 mins. If astronomical event is removed mean wait time is 30.91 mins. • Use NEWS and National Sepsis Screening tool to quickly identify the patient with Sepsis to standardise approach. • Competency/skills to recognise the Sepsis Patient. Prompt Recognition • Education/empowerment of ward staff re prompt communication to NCHD and escalation if no response to ensure patients are seen by a Doctor within the recommended time frame. • Develop standardise processes and clarity of roles. Timely Diagnosis • Ensure delivery of the Sepsis 6 within the 1st hour and continually monitor the patient to deliver the 3hr and 6 hr bundle. • Dedicated Sepsis consumables to hand. Early Intervention Continuous Learning • Review case studies and root cause analysis of events. • Ensure feedback to all the team. (
CUH SEPSIS Project Team • Sinéad Horgan and Grace Reidy • Project sponsor Dr Ken Walsh – Perioperative Clinical Director • Clinical lead Dr Dorothy Breen, Medical Lead Sepsis • Deirdre Feehely, Assistant Director of Nursing Perioperative Directorate • Roxana Mihu NCHD • Amudha Madhavan CNM2 • Staff Nurses • Healthcare Assistants Yvonne, Titus and Martha • Claire Costigan, CNM2 for the Deteriorating patient • Representation from Portering & laboratory. • Ciara O’Riordan, Ward Pharmacist. • Kelly Mc Carthy, Biomedical Scientist
Brainstorming session with staff: suggestions We need more education . Who should be aware? What about having a pack for sepsis? Trolley? Stickers- would they work? Poster ? Flyers? Who else needs to be involved? Champions? Pathways?
Working together on trolley NCHD input HCA’s stocking trolley Pharmacy list Trolley
PDSA 2: Introduction of Sepsis trolley Do • We worked with the ward staff,NCHD and pharmacist and they all agreed the content. • We were present on the ward during the first day to support the staff and encourage its use. • Everytime the trolley was used the NCHD ticked a sheet attached to the trolley, initialled it and put any comments on it . • The HCA on each shift took on board the stocking of the trolley Plan/Predict • To get 100% adoption of the trial “Sepsis Trolley” every time a patient triggers for sepsis on ward x • To have a dedicated space for the trolley with laminated stocklist. • To ensure the shelves are labelled and the MDT are involved. • Predict: It will be used for other deteriorating patients. • The trolley will not be replenished • The trolley will not be used Act • We needed to get a costing form procurement re a dedicated trolley. • We needed to streamline and communicate the information from the pharmacists • We needed to work with the labs also as we were aiming to initially improve the ward issues and need to focus on involving the labs.. • The HCA developed a checklist for the trolley • We will feedback to the team . • We need to get the trolley lock repaired.. • HCA requested that that we put a tie on the trolley which is broken when used to indicate it needs stocking Study • The trolley was used 2-3 times in the week. • We met with some of the NCHD’s and got their feedback. • They found it beneficial and reduced their time in gathering all the different inventory and wanted it to be used on other wards. • One NCHD said he used it for a deteriorating patient-not sepsis as it saved him time • The pharmacist gave us feedback on the replenishment of the IV antibiotics and what was needed for their information. The pharmacy want clear guidelines placed on the trolley re use of Meropenem • Feedback from the Staff/CNM was positive as they were not called away from the patient finding “stuff” for the NCHD. • The lock in the trolley is broken. • There was no document tray on trolley. • The AZO wipes were missing.
Conclusion • A reduction in Intensive Care admissions due to sepsis from this ward • A reduction in the patient’s length of stay by 33%. Cost of a ward bed day €1,316/day • Time to review went from 53 minutes to 30.9 minutes • Increased awareness of staff knowledge of sepsis