Download
1 / 22
220 likes | 395 Vues
Ascending thoracic aneurysm repair with CPB and circulatory arrest (case presentation). History. CC: 81 y.o. white male coming to ED after found in the bathroom. + LOC, no amnesia. Responsive on arrival. C/o stroke like symptoms: headache, confusion, left sided weakness,

E N D
Ascending thoracic aneurysm repair with CPB and circulatory arrest (case presentation)
History • CC: 81 y.o. white male coming to ED after found in the bathroom. + LOC, no amnesia. Responsive on arrival. • C/o stroke like symptoms: • headache, • confusion, • left sided weakness, • unable to turn the head to the left side
History cont.: • Allergy: Ciprofloxacin, Levaquin • PMHx: • HTN well controlled on Lisinopril and HCTZ • Type 2 DM well controlled by diet/exercise • Prostate cancer (on Megestrol) • Occasional CP (no AMI in the past) • COPD • PVD
History cont.: • PSHx: • Inguinal hernia repair • Umbilical hernia repair • Past Anesthesia Hx: • GA • No complications with GA
Physical: • HEENT: PEERL, EOMI • MP class 1, TMD 5 cm, Mouth opening 4 FB, good neck mobility, own dentition in a good shape • Cor: RRR, S1S2, no murmurs, no thrill, tones silent, distant on auscultation • Pulmo: decreased sounds bilaterally, no crackles or wheezing • Extremities: no gross abnormalities, left sided weakness • Neurological: AOx3, left sided focal signs • ASA 5, Case type: Emergency
Laboratory and studies report: • CBC: WBC=8.4, Hb=11, Hct=35, Plt=207 • Na=128, K=3.6, HCO3-=19, Cl=98, BUN=11, Creat=0.6, Glu=131 • Pt=12.0, PTINR=1.02, PTT=42.9 • ECG: NSR~100 BPM, nonspecific S-T changes, no signs of acute ischaemia • ECHO: 19 July 2002: EF 74%, no ischaemic changes • Adenosine myocardial perfusion test: 19 July 2002: NSR, left axis anterior hemiblock, mild S-T changes. No evidence of ischaemia. Normal test.
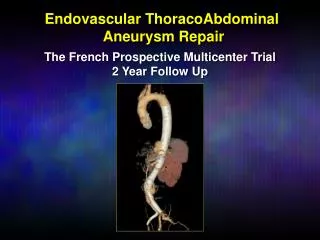
Ultrasound done in Oberlin hospital: Ascending Thoracic Aorta 45 mm Intimal flap
Ultrasound done in Oberlin hospital: Blood in dissection Type A ascending aortic aneurysm Aorta
Chronology: • Pt taken to OR 15. • Difficulty cross matching the blood • Anesthesia start time @ 20:28 with a-line and 2 large bore 16 G i.v. lines in place • Smooth i.v. induction: Fentanyl 100+150+200+250 mcg; Midazolam 5mg, Vecuronium 10 mg. • Easy ventilation and intubation; ET 8, Grade 1 view, atraumatic, secured @ 23 cm. • Left IJ 9 F introducer placed, PAC introduced, good waves and wedge detected, secured @ 54 cm. Patient tolerated procedure well. No complications. • Initial CI=2.4, SVO2=75%, CVP=14, PAP=24/14 mmHg
Intraoperative facts: • Maintenance of anesthesia before bypass: • Isoflurane 1.0%, O2 =2L, Air = 2L. • Fentanyl: 0.05 mcg/kg/min • Vecuronium: 3mg/h • Other drips: • Amicar • Sodium nitroprusside • NTG • Neosynephrine • BIS: ~ mid 40’s • BP titrated to a mean of 80’s • ABG @ the beginning surgery: pH=7.43, CO2=31.8, O2=207, HCO3=21.1, BE=-2.0, HCT=30, Na=123, K=3.4, Glu=160
Intraoperative during bypass: 1st time 2nd time 3rd time On pump 22:12 00:05 02:40 Off pump 22:56 01:48 04:05 • Circulatory arrest @ 22:35 = BIS 00 • Temperature during arrest: 18 C • MAP 15-20’s during circulatory arrest • ABG on the pump: pH=7.40, CO2=35, O2=336, HCO3=22, BE=-2.1, HCT=22, Na=123, K=3.8, Glu=167
Intraoperative events: • Proximal aortic graft required resuturing • Episode of hypotension/clotted pump filter • Marked reduction in systolic function after weaning from bypass • Unresponsive to iv epi/norepinephrine, but responsive to intracardiac Epinephrine 1 mg • Blood gas revealed PaO2=45 mmHg • Delayed reinstitution of CPB/clotted oxygenator
Intraoperative events (2): • Persistent lactic acidosis on bypass • Low urine output • Weaned from bypass, with persistent hypoxemia and lactic acidosis, and hematuria • Return to bypass for the 3rd time • Weaned from the bypass after 1 hour and 25 minutes • Blood clot removed from right atrium • Patient remained H/D unstable and expired @ 05:30
Intraoperative facts: • Total surgery time 20:28-05:02= 514 min • Total bypass time: 44min+103min +85 min= 232 min • Total circulatory arrest time = 27 minutes • EBL ~ 2000 ml • PRBC’s= 6 units • Platelets = 6 packs • Fluids: 2200 ml • Urinary output = 120 ml (hemolyzed) • Blood clot removed from right atrium • Patient expired 05:30 AM • CAA identified in the blood
Cold agglutinins antibody - CAA: • Common but usually unimportant - in serum of almost all healthy patients • AHA caused WAB = 1:85.000; caused CAA = 1:300,000 • Female/male = 1.5/1.0 • Associated with: • Infectious mononucleosis (60%) • Lymphoreticular neoplasms • Mycoplasma pnuemoniae • IgM autoantibodies against RBC I-antigen
Cold agglutinins antibody - CAA: • Thermal amplitude - blood temperature below CAA react • Higher thermal amplitude = more malignant CAA (35 Co) • Routine screen by blood banks for CAA @ 37Co • Significance of CAA is determined by: • Agglutination of RBC in 20 Co saline • Agglutination of RBC in 30 Co albumin • If tests are negative significant hemolysis is unlikely (Leach AB, Van Hasselt GL, Edwards JC:Cold agglutinins and deep hypothermia. Anesthesia 38:140;1983)
CAA - physical exam and distribution: • PE: may reveal • nothing unusual • pallor only, unless the patient is observed during or shortly after cold exposure. • purplish discoloration of the ears, forehead, tip of the nose, and digits may then be observed. • Distribution is provided by a study of 78 patients with persistent cold agglutinins: • 31 lymphoma (40%), • 24 chronic, idiopathic CAD (31%) • 13 Waldenström syndrome (16%) • 6 chronic lymphocytic leukemia (CLL) (8%) (Crisp, 1982)
CAA - Ddx: • DDX: • Cryoglobulinemia • Warm AIHA (Warm antibody–mediated autoimmune hemolytic anemia ) • Neoplasms • Drug-induced immune hemolytic anemia • Heparin-induced thrombocytopenia/thrombosis syndrome (HITTS) • Drug-induced hemolytic anemia • Infections
Management of CAA and CPB:. • Depends on : 1.titers, 2.thermal amplitude • 1) During the bypass RBC agglutination can be determined by mixing the blood with cold cardioplegia • 2) Dilute the blood sample to simulate the dilution with CPB and cool it down. (may not have the reaction) • Many institutions avoid hypothermic CPB if CAA present • Cold cardioplegia may produce agglutination in small heart blood vessels • If hypothermia required despite CAA • preoperative plasmapheresis to reduce titers • limit hypothermia to temperature exceeding thermal amplitude • use standard hemodilution techniques
Management of CAA and CPB:. • Cold cardioplegia with normothermic bypass and no plasmapheresis • normothermic CPB • cardioplegia 37 Co to washout CAA • 4 C cold cardioplegia • Malignant cold CAA • Consider total washout technique - exchange patient’s blood with donor’s blood • Heat all anesthetic gases, IV Fluids, blood, and plasma • Keep room warm • Use washed RBC’s