Delirium Monitoring in ICU: CAM-ICU Implementation Webinar
360 likes | 468 Vues
Join the webinar to learn about CAM-ICU, its importance in ICU settings, features, administration, case studies, and successful implementation strategies. Understand delirium impact on patient outcomes.

Delirium Monitoring in ICU: CAM-ICU Implementation Webinar
E N D
Presentation Transcript
Implementing the CAM-ICU April 19, 2012 The Webinar will begin at 2:00 PM PDT.
Implementing the CAM-ICU Michele Balas, PhD, RN, CRNP, CCRN University of Nebraska Medical Center
Implementing the CAM-ICU Michele C. Balas PhD, RN, APRN-NP, CCRN Assistant Professor University of Nebraska Medical Center, College of Nursing mbalas@unmc.edu
University of Nebraska Medical Center OBJECTIVES • Describe the importance of delirium monitoring in the ICU setting • Define the 4 delirium features assessed by the CAM-ICU • Demonstrate performance of CAM-ICU administration • Provide case studies of delirium assessment using the CAM-ICU • Discuss strategies for successful CAM-ICU implementation
University of Nebraska Medical Center ICU DELIRIUMWHY SHOULD WE CARE? • Incidence • 70-87% Mechanically ventilated ICU patients • 50-80% Surgical/Trauma/Burn ICU • 20-50% Non mechanically ventilated ICU • Outcomes • Independent predictor of higher ICU, hospital, & long-term mortality rates • 3 fold ↑ risk at 6 months • Each day delirious ↑ 10% mortality!!!!!!
University of Nebraska Medical Center ICU DELIRIUMWHY SHOULD WE CARE? • Outcomes • ICU & hospital LOS • Poor functional recovery • New institutionalization • Multiple complications • Long-term cognitive impairment • Cost • (38-152 BILLION $$ annually!!!!)
University of Nebraska Medical Center ICU DELIRIUMWHY SHOULD WE CARE? • 10-50% of all ICU survivors experience • PTSD • Depression • Anxiety • Sleep disorders • Need for caregiver assistance
THE PROBLEM……….. • Recognition • Weinert et al. (2007) CCM • 85% of 18,050 evaluations had sedation (N=274) • 1 in 3 unarousable (32%) • 1 in 5 no spontaneous motor activity (21%) • Only 2.6% of providers thought patients were “over-sedated”!!!!!!
University of Nebraska Medical Center WHAT IS DELIRIUM?-DSM IV DEFINITION • Disturbance of consciousness (i.e., reduced clarity of awareness of the environment) with reduced ability to focus, sustain or shift attention • A change in cognition or the development of a perceptual disturbance that is not better accounted for by a preexisting, established or evolving dementia • The disturbance develops over a short period of time (usually hours to days) & tends to fluctuate during the course of the day • There is evidence from the history, physical examination or laboratory findings that the disturbance is caused by the direct physiological consequences of a general medical condition
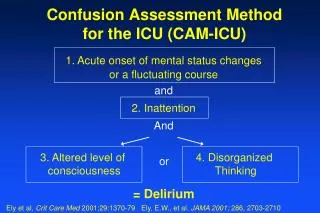
University of Nebraska Medical Center WHAT IS THE CAM-ICU • Bedside assessment tool intended for use by non- psychiatrists (i.e. ICU RNs, MDs, RTs, PT/OT) • Adapted from original CAM, for use in critically-ill, non-vocal (i.e. mechanically ventilated) patients • Delirium defined in terms of 4 diagnostic features • Feature 1-Acute onset or Fluctuating Course • Feature 2-Inattention • Feature 3-Altered level of consciousness • Feature 4-Disorganized thinking • Delirium is present when patient displays features 1 AND 2 and either 3 OR 4
University of Nebraska Medical Center TRUST MECAM-ICU QUICK & EASYLESS THEN 90 SECONDS TO ADMINISTER
University of Nebraska Medical Center STEP 1ADMINISTER RASS • Determine if you can even administer the CAM-ICU • Consciousness=arousal level + content • “Are the lights on?” • Use valid & reliable sedation/arousal tool (i.e. the RASS)
University of Nebraska Medical Center STEP 2ADMINISTER CAM-ICU • To every patient except if they are comatose (i.e. RASS -4 or -5) • You do NOT have to assess all 4 features (only those needed to determine if they are delirious) • Delirium= Feature 1 AND Feature 2 AND either Feature 3 OR 4 • Good news-you have already assessed for Feature 3
University of Nebraska Medical Center FEATURE 1MUST HAVE!!!!! • Has the patient had an acute change from mental status baseline? • OR • Has the patient’s mental status fluctuated during the past 24 hours? • __________________________________________ • If both of these questions are answered NO, STOP you are done. The patient is NOT delirious!
University of Nebraska Medical Center FEATURE 1MUST HAVE!!!!!FAQs • How do you determine mental status baseline? • Do you always use same baseline? • How do you handle a permanent change of baseline during hospitalization? • Does it still count as fluctuation if patient is receiving sedatives?
University of Nebraska Medical Center FEATURE 2MUST HAVE!!!!! • Inattention • “Squeeze my hand when I say the letter A” • SAVEAHAART • Errors=No squeeze with “A” & squeeze on letter other than “A” • Feature 2 is present if the patient has >2 errors • If inattention is NOT present, STOP you are done. The patient is NOT delirious!
University of Nebraska Medical Center FEATURE 2MUST HAVE!!!!! • Alternate Inattention Assessment- • Use of Pictures • Step 1-5 pictures • Step 2-10 pictures • Scoring
University of Nebraska Medical Center FEATURE 2MUST HAVE!!!!!FAQs • If the patient is RASS -3 or very lethargic, is the CAM-ICU unable to assess? Is the patient delirious? • Do I have to do both the letters & pictures on every patient? • How do I get the pictures? • Are there other letter sequences I could use to assess Feature 2?
University of Nebraska Medical Center FEATURE 3MUST HAVE EITHER THIS FEATURE OR FEATURE 4 • Altered Level of Consciousness • Assess with RASS • Feature is PRESENT when patient scores anything other than a RASS of O (i.e. alert) • If Features 1, 2 & 3 are deemed present, STOP you are done, the patient is delirious (CAM-ICU positive)
University of Nebraska Medical Center FEATURE 3MUST HAVE EITHER THIS FEATURE OF FEATURE 4FAQs • Is feature 3 positive in coma? • What is the difference between Feature 3 and Feature 1? • What if we use a different sedation assessment scale?
University of Nebraska Medical Center FEATURE 4MUST HAVE EITHER THIS FEATURE OF FEATURE 3 • Disorganized thinking • 2 steps • Step 1-Questions • Will a stone float on water? • Are there fish in the sea? • Does 1 pound weigh more than 2 pounds? • Can you use a hammer to pound a nail?
University of Nebraska Medical Center FEATURE 4MUST HAVE EITHER THIS FEATURE OF FEATURE 3 • Step 2-Command • “Hold up this many fingers” (Hold up 2 fingers) • “Now do the same thing with the other hand” (Do not demonstrate) • OR-“Add one more finger” (If patient is uanble to move both arms) • Feature 4 is present if there is >1 error for the combined Questions & Command • If Features 1, 2 & 4 are deemed present, STOP you are done, the patient is delirious (CAM-ICU positive)
University of Nebraska Medical Center FEATURE 4FAQs • How frequently do you have to assess for this Feature? • If the patient answers the 4 questions correctly, do you still assess the command? • Is there an alternate set of questions?
University of Nebraska Medical Center CASE STUDY #1 • Mrs G. is a 65 y/o admitted for acute respiratory failure. She lives independently in her own home, is active in her church, and still drives herself everywhere. You walk into the room and she looks at you immediately. She appears anxious as she is being ventilated with BIPAP. Her arms are restrained and she is pulling at them to get her BIPAP mask off. Her lowest RASS in the previous 24 hours was –2, and highest RASS was +2. She scored 5 on the Letters of Feature 2. She answers 2 questions correctly and follows the commands of Feature 4.
University of Nebraska Medical Center CASE STUDY #4 • You enter the room of a 78 y/o cardiac patient you have been seeing over several days. She lives at home and cares for her husband. She has been RASS -1 to 0 and CAM-ICU negative for the past 48 hours. She is RASS 0 this morning and greets you by saying “How do you think I look?” You exchange pleasantries about how she is doing today. She answers 2 questions correctly, follows commands but gets 6 letters and 5 pictures correct.
University of Nebraska Medical Center CASE STUDY #2 • Your 80 y/o patient was successfully weaned from the ventilator and extubated at 0800 after abdominal surgery. He is alert and calm since all sedation and analgesia had been stopped earlier in the morning. Yesterday evening and last night he had periods of agitation with a documented RASS of -1 to +3. He lives with family due to physical limitations with mobility but is still cognitively intact. He correctly answers all the questions and is able to identify the number of fingers the interviewer holds up and follows the command. He squeezes correctly on all the letters.
University of Nebraska Medical Center CASE STUDY #3 • You enter the room of a 65 y/o patient you enrolled 2 days ago after she had emergency abdominal surgery. She is still on the ventilator, her eyes are closed, she does not open her eyes to verbal stimuli but does respond to physical stimuli. She was on paralytics and has been off them for 24 hours. She is still receiving sedatives. She has been RASS -5 to -2 over the past 24 hours. She is unable to follow any commands. Prior to surgery she had just retired from her teaching job.
University of Nebraska Medical Center ISSUES IN IMPEMENTATIONFAQs • Can I use the CAM-ICU outside the ICU? • Can I use the CAM-ICU in my Neuro unit or with patients with TBI? • Can I perform a CAM-ICU on a patient with known dementia? • Can I use the CAM-ICU in patients having ETOH withdrawal?
University of Nebraska Medical Center ISSUES IN IMPEMENTATIONFAQs • How do I perform the CAM-ICU with non-English speaking patients? • How do you identify delirium in the depressed patient? • When should pharmacologic treatment for delirium be discontinued? • Is it necessary to assess for all 4 features of delirium on every patient?
University of Nebraska Medical Center ISSUES IN IMPEMENTATIONFAQs • How frequently should I administer the CAM-ICU? • My patient is CAM-ICU negative, but is still acting delirious. What does this mean? • Do I need to do all 4 Features in order? • How should I document the CAM-ICU? • Should I do the CAM-ICU before or after an SAT? • How do I know if my staff is performing the CAM-ICU correctly?
University of Nebraska Medical Center RESOURCES • All information contained in this presentation was retrieved from the website: www.icudelirium.org • CAM-ICU training manual • Case studies • Spot check forms • Example documentation forms • CAM-ICU/RASS pocket cards available upon request • Coming soon-“ICUsurvivors.com” • Supported by grant funds through the RWJF INQRI program
Cynosure Health SummitTHE GREAT QUALITY SWAP MEETBringing Nationally Renowned Innovation to Your Own Backyard May 21, 2012 SSF Conference Center