Download
1 / 32
330 likes | 891 Vues
AVR: Choice of Prosthesis. Tirone E. David University of Toronto. AVR: Choice of Prosthesis. “The perfect heart valve substitute is yet to be discovered”. AVR: Choice of Prosthesis. Mechanical valves are durable but require life-long anticoagulation

E N D
AVR: Choice of Prosthesis Tirone E. David University of Toronto
AVR: Choice of Prosthesis “The perfect heart valve substitute is yet to be discovered”
AVR: Choice of Prosthesis Mechanical valves are durable but require life-long anticoagulation Tissue valves do not require anticoagulation but they are not as durable
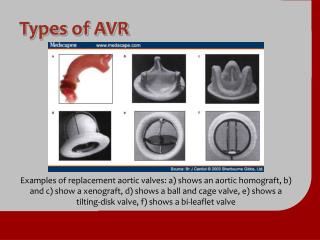
AVR: Choice of Prosthesis Mechanical Valves Tissue Valves Bioprosthetic Porcine Pericardial Biological: Aortic homograft Pulmonary autograft
AVR: Choice of Prosthesis Does the type of heart valve prosthesis affect patients’ survival? Randomized clinical trials
VA Randomized Trial Outcomes 15 Years After Valve Replacement With a Mechanical Versus a Bioprosthetic Valve: Final Report of the Veterans Affairs Randomized Trial Hammermeister K et al. - J Am Coll Cardiol 2000;36:1152-8 Between 1977 and 1982, 394 men undergoing AVR were randomized in the OR to receive either the Björk-Shiley spherical disc mechanical prosthesis or a Hancock porcine bioprosthetic valve
VA Randomized TrialLate Mortality After AVR 79±3% 66±3%
VA Randomized TrialCauses of Death After AVR Björk-Shiley Hancock Valve-related 37% 41% Cardiac-related 17% 21% Non-cardiac 36% 26% Undetermined 10% 12%
Edinburgh Randomized Trial Twenty year comparison of a Björk-Shiley mechanical heart valve with porcine bioprosthesis Oxenham H et al. – Heart 2003;89:715-21 Björk-Shiley mechanical vs. porcine bioprosthesis 541 patients ~54±10 years of age 211 – AVR 261 – MVR 61 – AVR+MVR
Edinburgh Randomized TrialPatients’ Survival After AVR Survival at 20 years: Mechanical = 28±4% Bioprosthesis = 31±5% All patients
AVR: Choice of Prosthesis • These two randomized trials used first generation bioprosthetic heart valves • The mechanical valve used is no longer available • Are the findings applicable to our practice today?
1st and 2nd Generation Bioprosthetic Valves Hancock - Stanford Hancock II - Toronto
AVR: Choice of Prosthesis Does the type of heart valve prosthesis affect patients’ survival? Retrospective clinical studies
AVR: Choice of Prosthesis Twenty-year comparison of tissue and mechanical valve replacement Khan S et al - J Thorac Cardiovasc Surg 2001;122:257-69 AVR: 666 patients with mechanical ~ 64 years of age 725 patients with bioprosthesis ~72 years of age
AVR: Mechanical vs BioprosthesisPatients’ Survival JTCVS 2001;122:257-69
AVR: Choice of Prosthesis Aortic valve replacement in patients aged 50 to 70 years: Improved outcome with mechanical versus biologic prostheses Brown ML, Schaff HV, et al – JTCVS 2008;135:878-84 1990 to 2000: 510 St. Jude +/- CABG and 257 CE +/- CABG Matched 1:1 - age, gender, CABG, valve size: 220 in each group
AVR: Choice of Prosthesis Mechanical Porcine p value Operative mortality 1.8% 5.5% 0.04 10-year events: Survival 72% 50% 0.01 Freedom from redo AVR 97% 91% 0.1 Incidence of major bleeding 14% 6% 0.06 Follow-up 92% complete Same proportion of cardiac deaths (heart + valve) JTCVS 2008;135:878-8
AVR: Choice of Prosthesis Risk-corrected impact of mechanical versus bioprosthetic valves on long-term mortality after aortic valve replacement Ole Lund and Martin Bland – JTCVS 2006;132:20-6 Mechanical Bioprosthetic Number of articles 15 23 Number of patients 8,578 8,861 Mean age in years 58 69 CABG 16% 34% Endocarditis 7% 2% Overall death/year 3.99% 6.33%
AVR: Choice of Prosthesis Risk-corrected impact of mechanical versus bioprosthetic valves on long-term mortality after aortic valve replacement Ole Lund and Martin Bland – JTCVS 2006;132:20-6 • RESULTS: • Patients’ mean age was directly related to death rates • with no interaction with valve type. • Death rate corrected for age, NYHA classes III and IV, • AI, and CABG and no interaction with valve • No differences in rates of thromboembolism.
AVR: Choice of Prosthesis Conventional wisdom: Survival after AVR is not affected by the type of aortic valve prosthesis
AVR: Choice of Prosthesis • Are valve-related complications dependent on the type of heart valve prosthesis?
VA Randomized TrialAVR: Morbid Events at 15 years Björk-Shiley Hancock p value Any valve-related complication 65±4% 66±5% 0.26 Systemic embolism 18±4% 18±4% 0.66 Bleeding 51±4% 30±4% 0.0001 Valve thrombosis 2±1% 1±1% 0.33 Endocarditis 7±2% 15±5% 0.45 Perivalvular regurgitation 8±2% 2±1% 0.09 Reoperation 10±3% 29±5% 0.004 Primary valve failure 0±0% 23±5% 0.0001
AVR: Choice of Prosthesis Performance of bioprostheses and mechanical prostheses Assessed by composites of valve-related complications to 15 years after aortic valve replacement V. Chan, WRE Jamieson et al. – J TCVS 2006;131:1267-73 • Study end-points: • Valve-related mortality • Valve-related morbidity • Valve-related reoperation
Mechanical vs. BioprosthesisFreedom from valve-related reoperations 51-60 years JTCVS 2006;131:1267-73
Mechanical vs. BioprosthesisFreedom from valve-related reoperations 61-70 years JTCVS 2006;131:1267-73
Mechanical vs. BioprosthesisFreedom from valve-related reoperations >70 years JTCVS 2006;131:1267-73
Performance of bioprostheses and mechanical prostheses Assessed by composites of valve-related complications to 15 years after aortic valve replacement V. Chan, WRE Jamieson et al. – J TCVS 2006;131:1267-73 Conclusion: No differences were observed in valve-related reoperation and mortality in patients >60 years. Comparative evaluation gives priority for bioprostheses in patients >60 years based on improved morbidity profile.
AVR: Hancock IIFreedom from Failure by Age ± Age 10 yr 15yr <65y 94 ± 2 72 ± 5 >65y 99 ± 1 99 ± 1 • Pts at risk • 250 162 61 • 704 442 202 25
Quality of LifeMechanical vs Bioprosthesis “Quality of life in patients with biological and mechanical prostheses. Evaluation of cohorts of patients aged 51 to 65 years at implantation” - Perchinsky et al. Circulation 1998;98:II-81-87. Study design: QOL in age and sex matched patients with mechanical and biological valve and general population SF-12 form & Lamy Smiley Faces form
Quality of LifeMechanical vs Bioprosthesis • Patients with mechanical valves were troubled with noise, bleeding and blood tests (p<0.01) • Patients with bioprosthesis were troubled with prospect of reoperation (p<0.01) • No difference in fear of valve failure • QOL similar in both groups and general population • 97% would make the same choice of valve Perchinsky et al. Circulation 1998
Quality of LifeMechanical vs Bioprosthesis Conclusions: • Human beings are resilient and adaptable • Most patients with prosthetic heart valves are well adjusted to their condition
AVR: Choice of Prosthesis • Patients’ age is probably the most important factor in recommending tissue or mechanical valve • Bioprosthetic valves are ideally suitable for older patients (>70 years) or those who are not likely to outlive the valve (co-morbidities) • Mechanical valves should be recommended to younger patients (<60 years) • If anticoagulation is a perceivable problem, tissue valves can be used in younger patients but the probability of reoperation is high