Download
1 / 39
530 likes | 1.07k Vues
Cathy Meaney NE Thames Regional Molecular Genetics. Non-invasive prenatal sex determination & single gene disorder testing using cell-free DNA. Great Ormond Street Hospital for Children NHS Trust. Prenatal Diagnosis. Invasive techniques amnio, CVS, PGD risks, sampling time, costs

E N D
Cathy Meaney NE Thames Regional Molecular Genetics Non-invasive prenatal sex determination& single gene disorder testing using cell-free DNA Great Ormond Street Hospital for Children NHS Trust
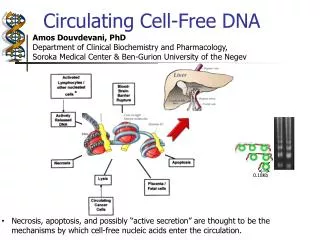
Prenatal Diagnosis Invasive techniques amnio, CVS, PGD risks, sampling time, costs Non invasive prenatal diagnosis 1989 fetal cells in maternal blood Low number (1-6 cells/ml blood) Fetal cell enriching and isolation - time consuming Labor intensive or difficult on large scale Low sensitivity PND Cells can remain in circulation for many years > confusion as to which pregnancy testing 1996 cell-free tumour DNA Found in plasma & serum from cancer patients Monitor treatment without BMT for karyotyping
1997 cell-free fetal DNA Gestation Period Early Late Genome Equivalents (G.E.) / ml maternal plasma 25.4 292.2 % fetal DNA of total DNA in maternal plasma 3.4% 6.2% • Lo et. al. > maternal plasma contains both fetal & maternal DNA • Fetal DNA is stable & in high concs in maternal plasma • Cleared rapidly from maternal circulation following birth (with a half-life of minutes) NB. Genome equivalent obtained using conversion factor of 6.6pg of DNA/cell • Likely that circulating fetal DNA released from fetal and/or placental cells undergoing apoptosis • Syncytiotrophoblasts in the form of apoptotic fragments packaged into microvesicles • Ties in with observed different sizes (fetal < 300bp and maternal > 350bp) • Detect fetal abnormality without invasive procedure • ? problems with multiple pregnancies
Clinical Applications Blood typing Genotyping Rh-ve women Fetus could inherit RhD allele from father Fetal sexing (detecting Y chromosome sequences eg. SRY, DYS) X-linked diseases CAH (pregnant women get dexamethasone for CAH female fetuses) STRs for fetal alleles, trisomy 13, 18, 21 Fetal aneuploidy detection (T21 >2-fold increase in total fetal cfDNA) Pregnancies at risk for pre-eclampsia > increase in cell-free fetal DNA Single gene disorders Achondroplasia, myotonic dystrophy, prenatal exclusion in CF, beta-thalassaemia
Challenges Sensitivity Early detection when fetal DNA at low levels (1gE/PCR) Specificity Low amount of fetal DNA (1-6%) in high background of maternal DNA Dynamic Range 1-560gE/ml fetal DNA and 70>4000gE/ml total DNA Lack of reliable fetal-specific markers Confirm presence of fetal DNA Mother & fetus share, on average, half of their genomic DNA seq’s Only detect uniquely fetal DNA sequences that are paternally inherited Technology / platforms Real time PCR, SABER MALDI-TOF MS
Extraction of cell-free DNA PLASMA 6-10mls (cell-free maternal & fetal DNA) 1 ml plasma aliquots > store -20C Extract DNA using Qiagen QIAamp MinElute Virus Kit (manual or EZ1 robot) Elute into 50-100l RNAse free water 16-20mls maternal EDTA blood from 7 weeks gestation (pref within 24hrs) Spin blood at 3000g plasma MBC RBC BUFFY COAT (maternal white blood cells) Extract DNA on EZ1 robot or manual salting out method
Real-Time PCR Fetal sex determination Polymorphic markers Achondroplasia common mutation
Cycle Cell-Free fetal DNA analysisusing Real Time PCR Theoretical • Real-Time PCR allows us to ‘see’ the exponential phase so can calculate how much DNA started with • Closed system – contamination • Probes - specificity, sensitivity • Melt curve analysis - primer • dimer & mis-priming • Optimisation • Reagent cost • Multiplex Log Target DNA Real Life Ct Threshold Cycle, Ct The point at which fluorescence rises appreciably above background
End Point Measurements 96 replicates of the identical reaction can have very different final amounts of fluorescence
Taq Polymerase Reporter Reporter Quencher Target Sequence Fluorescent Tag Taqman probes • A hybridization probe is constructed with a fluorescent reporter • at one end to a nearby quencher. • The reporter is excited but its emitted fluorescence is captured • by the nearby quencher. • No reporter fluorescence is detected. During the extension step, the polymerase encounters the TaqMan probe and chews off the end. • Once freed from the quencher the reporter fluorescence can be detected indicating amplification has occurred
Fetal sex determination using Real Time PCR Machine Y specific primers/probe Control primers/probe Source iCycler (Biorad) AMEL Y (FAM) & SRY (HEX) AMEL X (ROX) In-house design iCycler (Biorad) DYS (FAM) (multicopy pseudogene) CCR5 (FAM) Published sequences AB 7300 (Applied Biosystems) SRY(FAM) CCR5 (FAM) AB Assay-on-Demand Kits
Fetal sex determination on AB 7300 Applied Biosystems Assay-on Demand kits 60°C annealing temp (95°C/10’, 50 cycles of 95°C/15 sec and 60°C/1min) • Separate assays; • SRYprimers and probe (FAM) specific for • Y chromosome sequences • CCR5primers and probe (FAM) as control • for total DNA measurement • 20ul PCR reaction in 96 well microtitre plate • AB Universal Mastermix • Store primers & probes in small aliquots in • freezer & use once • Accurate pipetting using filter tips • Plastic seal, spin plate, no bubbles
Plate Setup 1 2 3 4 5 6 7 8 9 10 11 12 A SRY ffDNA 1 SRY ffDNA 1 SRY ffDNA 1 SRY ffDNA 1 SRY ffDNA 1 SRY ffDNA 1 CCR5 ffDNA 1 CCR5 ffDNA 1 B SRY ffDNA 2 SRY ffDNA 2 SRY ffDNA 2 SRY ffDNA 2 SRY ffDNA 2 SRY ffDNA 2 CCR5 ffDNA 2 CCR5 ffDNA 2 C SRY ffDNA 3 SRY ffDNA 3 SRY ffDNA 3 SRY ffDNA 3 SRY ffDNA 3 SRY ffDNA 3 CCR5 ffDNA 3 CCR5 ffDNA 3 D SRY ffDNA 4 SRY ffDNA 4 SRY ffDNA 4 SRY ffDNA 4 SRY ffDNA 4 SRY ffDNA 4 CCR5 ffDNA 4 CCR5 ffDNA 4 E SRY ffDNA 5 SRY ffDNA 5 SRY ffDNA 5 SRY ffDNA 5 SRY ffDNA 5 SRY ffDNA 5 CCR5 ffDNA 5 CCR5 ffDNA 5 F SRY control Male S4 SRY control Male S4 SRY control Male S4 SRY control Female SRY control Female SRY control Female SRY control H20 SRY control H20 SRY control H20 CCR5 control H20 CCR5 control H20 CCR5 control H20 G SRY control Male S4 SRY control Male S4 SRY control Male S4 SRY control Female SRY control Female SRY control Female SRY control H20 SRY control H20 SRY control H20 CCR5 control H20 CCR5 control H20 CCR5 control H20 H CCR5 Male S1 100ng CCR5 Male S1 100ng CCR5 Male S1 100ng CCR5 Male S2 10ng CCR5 Male S2 10ng CCR5 Male S2 10ng CCR5 Male S3 1ng CCR5 Male S3 1ng CCR5 Male S3 1ng CCR5 Male S4 0.1ng CCR5 Male S4 0.1ng CCR5 Male S4 0.1ng
Amplification Plots of SRY & CCR5 SRY CCR5 DRn S2 S3 S4 S1 ffDNA S1 S4 S2 S3 ffDNA Standard Curves S4 S4 CCR5 SRY S3 S3 S2 S2 S1 S1
Positive result (PCR amplification with SRY) Replicates with Ct < 40 cycles indicating male fetus Negative result (no PCR amplification with SRY) Replicates with Ct > 40 cycles (or no amp) indicating female fetus Negative controls Female DNA and H20 control wells with Ct value > 40 Positive controls Male DNA replicates amplify with Ct < 40 Slope of standard curves Values between –3.3 and –4.5 Repeat if discrepancies RQ-PCR Results Validation
Examples of X-linked diseases tested Metabolic (Fabry, Hunters) X-linked immunodeficiencies (Wiskott Aldrich sydrome, XSCID, XL-CGD) X-linked Adrenoleukodystrophy (ALD) Haemophilia DMD/BMD X-linked icthyosis Menkes Retts Ambiguous genitalia CAH
PolymorphicMarkers • SRY negative result • True female result or low circulating fetal DNA concentrations or fetal DNA loss during sampling processing? • Panel of 8 biallelic markers tested by RQ-PCR • Detect fetal markers not present in maternal DNA to confirm presence of fetal DNA Maternal EDTA - neg for S03, S04, S05, S06 Plasma - positive for marker S05
RASSF1A universal marker • RASSF1A promoter • hypermethylated in placenta (>fetus) • hypomethylated in maternal blood cells (Lo et. al. 2007) • Use BstU1 methylation sensitive restriction enzyme to digest unmethylated maternal DNA • amplify with RASSF1A primers/probe • detection of placental-derived hypermethylated RASSF1A sequences in maternal plasma
SAFE QC Workshop 2:Showing the quality of performance of non-invasive prenatal genotyping in Europe 0.6 ml plasma sent out at RT 18 laboratories received 4-6 samples each Tested for RhD & SRY Results on 105 RhD and 109 SRY Correct results: 193 (90.2%) False results: 10 (4.7%) 6 false positive and 4 false negative Inconclusive results: 11 (5.1%) 8 in positive samples and 3 in negative samples
Total samples tested = 39 Samples (sex confirmed n=25) Sensitivity (% Male pregnancies predicted as male) 12/12 (100%) Specificity (% Female pregnancies tested negative for female pregnancy) 11/13 (85%) Fetal sexing results unconfirmed (i.e. by US, amnio, birth) 12 Miscarriage 2 Fetal sex results: 2006-2007
False positives CAH - 5 & 6 weeks gestation ? Contamination strict validation criteria repeat test on a 2nd aliquot of plasma request 2nd EDTA sample Risk of FP due to sex discordant DZ vanishing twins is 1/70 Early good sonography More wary in assisted pregnancies and mothers with higher incidence DZ twins
2007-2009 Samples > 7 weeks gestation About 190 patients tested Of those samples there were repeat samples or 2 samples tested at same time
Single Gene Disorders Skeletal Dysplasia Achondroplasia Craniosynostosis Apert syndrome Crouzon syndrome Torsion Dystonia
Achondroplasia Applied Biosystems Assay-by-Design for SNP genotyping assays Taqman MGB labelled probes (FAM & VIC) using real time PCR Designed for genotyping specific SNPs Each assay enables scoring of both alleles in a single well Confidence levels are low for detecting fetal mutant DNA in maternal background enrichment of fetal DNA required fetal DNA <350bp, maternal DNA >350bp
Achondroplasia - G380R g>a Extracted DNA from 400ul & 800ul plasma from mother with known ACH pregnancy Digested with BsrGI enzyme ⌐ 400ul plasma¬ ⌐ 800ul plasma¬ Ladder Uncut 5ul DNA 10ul DNA 20ul DNA 5ul DNA 10ul DNA 20ul DNA Normal control G380Rg>a control H20 132bp 112bp
Early-onset primary dystonia (DYT1) Usually presents in childhood or early adolescence with a minority occurring as an adult Dystonic muscle contraction causing uncontrolled distortion of parts of the body Regardless of ethnicity, majority of DYT1 patients have a 3bp GAG deletion (c.907_909delGAG / p.Glu303del) in exon 5 of TOR1A (encodes torsinA) Autosomal dominant disease with reduced penetrance ~ 30-40% of offspring from an affected or asymptomatic parent develop symptoms ~ 70% of mutations are parental derived with remaining de novo
DYT1 family Family; Father known to carry the common DYT1mutation [c.907_909delGAG (p.Glu302del)] Mother not tested Invasive PND on CVS DNA for first pregnancy PND requested for subsequent pregnancies Maternal plasma samples taken for non-invasive testing; 2nd pregnancy (7+5 weeks and 8+5 weeks gestation) 3rd pregnancy (7+3, 8+3 and 9 weeks gestation) Spin 16-20 mls EDTA blood (within 24 hrs) plasma extract cfDNA using manual Qiagen Virus MinElute spin column kit
Confirm mutation status in parental genomic DNA Tested maternal gDNA to confirm mother did not carry mutation (only detect uniquely fetal DNA sequences that are paternally inherited or de novo) Tested paternal gDNA to verify previous 3bp deletion heterozygote result Confirm presence of fetal DNA in extract Fetal sexing on cell-free DNA extract by real-time PCR; SRY not present consistent female fetus presence of fetal DNA could not be confirmed in cfDNA extract
DYT1 mutation detection c.907_909delGAG (p.Glu303del) in cfDNA • Designed primers for short PCR product • Run on 12% ATTO gel cfDNA Mother gDNA Pos cont Blank H20 cont Pos cont Wild type cont Blank H20 cont cfDNA cfDNA Mother gDNA Father gDNA 80bp 77bp 7+5 weeks 8+5 weeks
Confirmation on fetal tissue Sample from fetal tissue; confirmed the heterozygous c.907_909delGAG (p.Glu303del) mutation result from testing maternal plasma Ladder Fetal tissue Fetal tissue Maternal gDNA Pos cont (het) Wildtype Blank H20 control Heteroduplex 80 bp 77 bp
Single gene disorders tested Disease Gene Patient Gestation Result SRY RQPCR ACH FGFR3 1 33+2 Mutation present Not tested Gly380Arg 2 35 Mutation present Not tested (c.1138G>A) 3 32 Fetus unlikely to carry mutn Not tested 4 34 Mutation present SRY present Crouzon FGFR2 Ser347Cys 5 12+6 Fetus unlikely to carry mutation Not tested Apert FGFR2 Ser252Trp 6 (P1) 29+3 32+3 Mutation present Not tested (c.755C>G) 6 (P2) 16 Fetus unlikely to carry mutn SRY present DYT1 TOR1A 3bp del 7 (P1) 7+5 8+5 Mutation present (confirmed in fetal tissue) SRY not detected (Glu303del) 7 (P2) 7+3, 8+2, 8+6 Mutation present (confirmed in fetal tissue) SRY not detected 7 (P3) 7+5 8+5 Mutation present (confirmed in fetal tissue) SRY present
SGD testing conclusion Analysis using PCR/polyacrylamide gel does not have sensitivity compared to RTqPCR or MS high specificity due to the detection of what can only be a paternally derived fetal mutant allele in the maternal plasma Primers designed short PCR fragments < 200bp amplification of smaller-sized fetal cfDNA more efficient Advantages of using this method are simplicity, low costs and rapid results
SUMMARY Fetal sexing NIPD for fetal sexing using cfDNA successfully introduced as a service from 7 weeks gestation for XL diseases & CAH Quality control Quality controls in place, SAFE QC workshops Minimised false +/-ve’s by testing 2 samples a weeks gestation apart if < 9 weeks & 2 samples simultaneously if > 9 weeks Maximise amount of cfDNA yield Confirmation of presence of fetal DNA in cfDNA extract Polymorphic markers used for female predicted (SRY negative) results were laborious & not always informative Fetus specific (? RASSF1A) & disease specific markers Single gene disorders NIPD testing set up for some skeletal dysplasias/cranio & DYT1
Future Paternally derived or de novo mutation detection > enrichment of fetal DNA and higher cfDNA yield (as high background of maternal DNA interferes with detection) Develop fetal and disease specific markers for confirming presence of fetal DNA in extract
Future (cont) Detect maternally or paternally derived mutations with new technologies such as digital PCR and whole gen sequencing; Digital PCR (Lo et al, Fan) NA sample is extremely diluted & parallel PCRs undertaken so most reactions contain either a single or no target molecule Digital readout from microfluidic chip with 9180 (12x765) 6nl reaction wells where PCR is either -ve or +ve Correlates to absence or presence of target molecule Statistical analysis of proportion of +ve reactions among the total number of PCRs analysed allows measurement of number of target molecules in input sample Detection of Downs & b-thalassaemia in fetus and LOH in tumour samples and plasma of cancer patients
High through-put shotgun sequencing – Lo et al; Fan (massively parallel whole genome sequencing) Sequence cfDNA on average, 5 million sequence tags per patient sample Measure number of sequence tags mapped to each chromosome over or underrepresentation of any chromosome in maternal plasma DNA contributed by an aneuploid fetus Polymorphism-independent & therefore universally applicable for NIPD of fetal aneuploidy said to be more sensitive that digital PCR Fan et al., successfully identified all 9 x T21, 2 x T18 & 1 x T13 in a cohort of 18 normal & aneuploid pregnancies 14th week gestation earliest
Acknowledgements Laboratory (Regional Molecular Genetics) Gail Norbury Bhaneeta Mistry Lighta Godinho Clinical (Fetal Medicine Unit, UCH) Lyn Chitty Melissa Whitten Taita Stojilkovic Louise Thomasson Technical (Bristol) Kirsten Finning, IBGRL