Download

1 / 18
190 likes | 548 Vues
Current treatment of acute coronary syndrome 林口長庚醫院 心臟內二科 謝宜璋醫師 March,6, 2012. 狹窄. 閉鎖不全. 心臟病. 肥厚性. 冠狀動脈疾病 (缺血性疾病) 瓣膜疾病 心臟衰竭 心肌病變 心律不整 心包膜疾病 先天性心臟病 (心房,心室中膈缺損 ----- ). 擴張性. 心博過速. 心博過慢. Coronary Artery Disease (CAD). Etiology:

E N D
Current treatment of acute coronary syndrome 林口長庚醫院心臟內二科 謝宜璋醫師 March,6, 2012
狹窄 閉鎖不全 心臟病 肥厚性 冠狀動脈疾病(缺血性疾病) 瓣膜疾病 心臟衰竭 心肌病變 心律不整 心包膜疾病 先天性心臟病(心房,心室中膈缺損-----) 擴張性 心博過速 心博過慢
Coronary Artery Disease (CAD) Etiology: • Atherosclerotic disease of epicardial coronary arteries. • Luminal narrowing by other mechanism, e.g. coronary spasm, dissection of aorta, etc. • Embolization. • Arteritis of coronary arteries, e.g. Granulomatous disease, kawasaki syndrome, SLE, RA, etc. • Trauma to coronary arteries. • Intimal proliferative disease, e.g. amyloidosis, homocystinuria, etc.
Risk factors for CAD • Male • Ageing • Hypertension • Diabetes Mellitus • Smoking • Obesity • Dyslipidemia • Family history • Sedentary • Uremia • Homocysteinemia
CAD--- Symptoms • Exertional chest discomfort (squeezing, pressure, heaviness sensation) --- typical • Crescendo-decrescendo pattern • May radiate to the left shoulder, both arms, back, neck, or jaw • Lasting 1-10 minutes, if AMI30 mins • Relieved by rest or sublingual NTG, or not
Diagnosis of CAD • History: typical symptoms • Physical exam: non-specific signs • Laboratory: Resting EKG (electrocardiogram) Exercise treadmill test Thallium-201 scan Dobutamine stress test (echo) Multi-slices CT Angiogram (coronary)
CAD --- Management • Explanation and reassurance • Reduction of risk factors: Hypertension, Diabetes, dyslipidemia, smoking, exercise--- • Treatment of coexisting condition capable of aggravating angina • Adaptation of activities • Drug therapy • Mechanical revascularization (PCI): PTCA, stenting, atherectomy, etc. • Coronary artery bypass surgery (CABG)
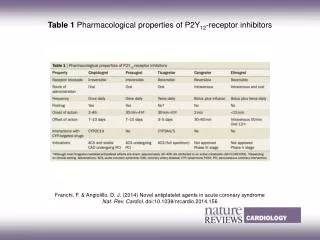
CAD --- Drug therapy • Antiplatelet agents: Aspirin, Clopidogrel • B-adrenoreceptor blockade: Propranolol, Atenolol, Nadolol, Bisoprolol , Carvedilol, Metoprolol • ACEI/ARB • Statin • Nitrate • Ca-channel blockers: Diltiazem, Nifedipine.
Clinical Manifestation of CAD (IHD) • Asymptomatic (silent ischemia) • Chronic stable angina pectoris • Acute coronary syndrome (ACS): unstable angina, non-ST elevation myocardial infarction (NSTEMI) • ST-elevation myocardial infarction (STEMI).
Acute Coronary Syndrome - Nomenclature Acute Coronary Syndrome No ST elevation ST elevation NSTEMI Unstable Angina ST elevation Myocardial Infarction JACC 2000;36:970-1062
STEMI--- Diagnostic Criteria • Typical chest pain • Serial ECG changes • Serial cardiac enzymes changes - At least fulfill 2 items in the above 3 criteria
STEMI --- Management (1) • Admit to coronary care unit • Absolute bed rest • Reperfusion therapy - Pharmacologocal: thrombolytic therapy - Mechanical: Primary PTCA, stenting • Drug therapy: - Analgesia, sedation - Oxygen - Anti-platelet agent and anticoagulants - B-blockers - Angiotensin-converting enzyme (ACE) inhibitor/ARB - Antiarrhythmic agents
Unstable Angina • New onset (< 2 months) angina • Accelerating angina (severity, frequency) • Resting angina • Pathophysiology: - progression of atherosclerosis - platelet aggregation - thrombus formation - changes in vasomotor tone (spasm)
Current therapy in acute coronary syndrome (UA / NSTEMI) • Bed rest, oxygen, opiate analgesics to relief pain, and anti-ischemic drugs (nitrates, β –blockers, calcium antagonists),CCU admission • Aspirin • IV heparin or SQ low-molecular-weight heparin • Clopidogrel/Prasugrel/Ticagrelor • IV platelet glycoprotein IIb/ IIIa antagonist • Percutaneous coronary interventions (PCI),CABG • ACE inhibitor • Statin
2007 ESC NSTE-ACS Guideline Update Key Recommendation on Clopidogrel Therapy • Clopidogrel • For all patients, immediate 300 mg loading dose of clopidogrel is recommended, followed by 75 mg clopidorel daily (I-A). Clopidogrel should be maintained for 12 months unless there is an excessive risk of bleeding (I-A). • For all patients with contraindications to aspirin, clopidogrel should be given instead (I-B). • In patients considered for an invasive procedure/PCI, a loading dose of 600 mg clopidogrel may be used to achieve more rapid inhibition of platelet function (IIa-B). • In patients pretreated with clopidogrel who need to undergo CABG, surgery should be postponed for 5 days for clopidogrel withdrawal if clinically feasible (IIa-C). Task Force Members et. al, European Heart Journal 2007;28(!3):1598-1660
2007 ACC/AHAUA/NSTEMIGuideline Update : Key Recommendations on Anti-plateletTherapy • Medical therapy without stenting • ASA 75-162 mg/d indefinitely (Class I, A) • Clopidogrel 75 mg/d, at least 1 mo (Class I, A), ideally up to 1 yr (Class I, B) • Bare metal stent • ASA 162-325 mg/d at least 1 mo, 75-162 mg/d indefinitely (Class I, A) • Clopidogrel 75 mg/d, at least 1 mo (Class I, A), ideally up to 1 yr (Class I, B) • Drug-eluting stent • ASA 162-325 mg/d at least 3 (sirolimus)-6 (paclitaxel) mo, 75-162 mg/d indefinitely (Class I, A) • Clopidogrel 75 mg/d > 1 yr (Class I, B)
Conclusions • CAD is an important, life-threatening disease • Risk factors control/life style modification are the best policy for prevention • Typical symptom is the keypoint for diagnosis, which can be confirmed by (non)invasive tests • Medications include anti-platelet agents, beta-blocker, ACEI/ARB, statin, nitrate • ACS should be treated early and aggressively • For STEMI patients, primary PCI (angioplasty) is better than thrombolysis • CABG is preserved for complicated/complex patient • Early detect and early treatment are crucial for CAD