Download
1 / 25
250 likes | 382 Vues
Integrated Multi-Level Approaches to Asthma Management. Noreen M. Clark, Ph.D. Dean & Marshall H. Becker Professor University of Michigan School of Public Health Director, Allies Against Asthma. Asthma Continues as a Major Public Health Problem.

E N D
Integrated Multi-Level Approaches to Asthma Management Noreen M. Clark, Ph.D. Dean & Marshall H. Becker Professor University of Michigan School of Public Health Director, Allies Against Asthma
Asthma Continues as a Major Public Health Problem • In 1997, 27 million people reported at some time of their life being diagnosed with asthma. • Asthma affects 5% to 10% of children under 18 years of age; is most common reason for childhood hospitalizations. • Asthma-associated work absence days have increased NHIS 50% since 1980 to (14 million in 1996). • In 1990, cost of illness related to asthma $6.2 billion, ($1.6 for inpatient hospital services alone). (Mannino et al, 2002) (Weiss et al, 1992)
MODERN PARADOX (1) • Understanding of the pathogenesis and treatment of asthma has increased • Morbidity and mortality from asthma have increased worldwide
MODERN PARADOX (2) • Understanding of the steps that can be taken to prevent severe asthma has increased • Emergency visits and hospitalizations for asthma have increased worldwide
Some Logical Conclusions • Patients and families are not managing asthma effectively • Clinicians are either not providing state of the art care, or, if they are, patients are not adhering to the recommended programs • The systems in which patients receive and health professionals provide services and education do not foster effective asthma management
Recognized Deficiencies in Health Care Systems • irregular or incomplete assessment or inadequate follow-up • inadequate or inconsistent patient education and feedback • omission of effective interventions or use of ineffective ones • failing to detect or inadequately manage a patient’s psychosocial distress (Wagner 1996a, 21)
Lack of Attention to Environmental Factors • Environmental tobacco smoke (ETS) is associated with the development of asthma. • ETS, cat, cockroach, dust mite are associated with the exacerbation of asthma in sensitive individuals. Institute of Medicine, National Academy of Sciences. 2000. Executive Summary. Clearing the Air: Asthma and Indoor Air Exposures. Washington, DC: National Academy Press.
Inadequate Insurance Coverage • Type of health care visits covered • Preventive services covered • Devices and equipment covered
Asthma is a very variable disease and an individual must exercise a significant degree of judgment regarding management.
Until we can prevent asthma as a disease, or develop a cure, success in control rests on • Removing systemic barriers to effective management • Positioning individuals to be the best possible manager of the condition
When stakeholders in asthma control come together to develop community wide solutions, the patient’s efforts to manage must be at the center of their strategies.
Management by Patient Family Involvement Clinical Expertise Work/School Support Community Awareness, Support & Action Community-Wide Environmental Control Measures Conducive Policies 16
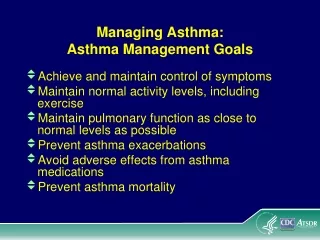
Intended outcomes of multi level approaches to asthma control: • Patients experience no or few symptoms • Patients are fully functioning • Morbidity decreases
Creating optimum opportunity for management and prevention of asthma symptoms depends on coordination among stakeholding individuals, organizations, and systems.
What should be the goal of community-wide coordination? • Individuals with asthma: access to continuous and consistent health care as well as ongoing information and support from providers, schools, employers and family • Health providers: standardized clinical care (including documentation) and links with external resources (schools, community) providing support and education for patients. • Health plans/insurers: Support for proven interventions to achieve uniformity in asthma management and appropriate health service use.
Schools/School Nurses/Child Care Providers: Ongoing Asthma education, communication with families, supportive care coordination with clinical providers, attention to indoor environmental issues. • Public Health Agencies: Availability of comprehensive data, strategic planning, formulating enabling policies, and coordination of efforts.
Reaching these goals depends on communication and integration of efforts across the sectors, and systems essential to asthma control.
State and local health departments can be primary facilitators of integration.
For example: Michigan state-wide action plan for asthma • engaged in an inclusive planning process • involves 125 representatives from public and private agencies and organizations • utilizes work groups that cross sectors • Clinical Care • Education • Environmental Quality • Surveillance & Epidemiology • recognizes and supports coalitions as the “engine” for integration
Michigan Asthma Strategic Planning Task Force • Provides support for coalitions including financial and technical assistance, networking, visibility. • Provides a structure for asthma champions from local communities to share information, identify and respond to changing priorities, and explore strategies feasible for their communities. • Coordinates internal public health and external resources to address asthma priorities. • Utilizes interdisciplinary teams (epidemiology, public health, environmental control, health education, health services, etc.) to plan and implement asthma solutions.
The key is integration. How to achieve it will differ by community. Coalitions may be key in the process.
Coalitions can enhance coordination and integration because by definition they cross sectors and systems. Over 200 asthma coalitions in the US. At least 20 in the midst of careful evaluation of collaborative processes and health outcomes.
Allies Against Asthma Resource Bank …a searchable on-line collection of resources including: • Asthma related educational materials • Asthma program resources • Asthma-related evaluation/survey instruments • Coalition-related materials Provides information about tools and resources and contact information to access. www.asthma.umich.edu/resourcebank
An integrated approach to asthma control could create procedures and linkages that enhance community capacity to manage other health problems.
Allies Against Asthma A national program supported by the Robert Wood Johnson Foundation with direction and technical assistance provided by the University of Michigan, School of Public Health