Beyond the first line : mTOR inhibitors
Beyond the first line : mTOR inhibitors. Viktor Grünwald Clinic for Hematology , Hemostasis , Oncology and Stem cell transplantation. The optimal sequence in RCC: But what patient , which drug ?. Validated in clinical trials. Everolimus. TKI. Currently under investigation. TKI.

Beyond the first line : mTOR inhibitors
E N D
Presentation Transcript
Beyondthefirstline: mTORinhibitors Viktor Grünwald ClinicforHematology, Hemostasis, Oncology and Stemcelltransplantation
The optimal sequence in RCC: Butwhatpatient, whichdrug? Validated in clinicaltrials Everolimus TKI Currentlyunderinvestigation TKI TKI
PFS: Everolimus - RECORD-1centralreview 100 Everolimus (n=277; Median PFS: 4.90 mo) Placebo(n=139; Median PFS: 1.87 mo) 80 HR = 0.33 (95% CI: 0.25, 0.43) Log-rank P<0.001 60 Proportion surviving, % 40 20 0 6 12 14 0 2 4 8 10 Month Motzer, et al. Cancer. 2010
Why do wedebateaboutthe optimal 2ndlinetherapy? • Pro (mTORi): • Phase III evidenceforeverolimusafterfailure of VEGF-targetedagents • Good tolerability • Change of mode of action (MOA) • Con (mTORi): • Somepatients will derivebenefitfromsustainedVEGFR-inhibition • Onlyfewobjectiveremissionswith mTORi • Isthereactivityafterfailure of everolimus?
mTOR binds in two distinct comlexes Wullschleger Cell 2006
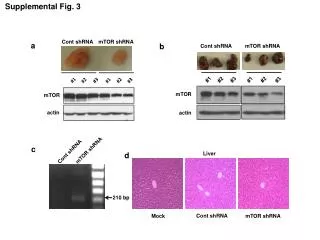
Resistance to mTORi – role of AKT escapeduring mTORC1 inhibition • PTEN-transfected PC3 cells • Unpublished data Rapamycin - - + 10%FBS - + + pAKT pp70s6k Actin
mTORInhibitors (mTORi) 2.0 Hudes NEJM 2007. MotzerLancet 2008. Desai et al. JCO 2005 23s: #3043. Wagner et al. Mol CancerTher 2009; 8(12s): #B141. Mol CancerTher 2009; 8(12s): #B141. Mallon et al. Mol CancerTher 2009; 8(12s): #B142. Jessen et al. Mol CancerTher 2009; 8(12s): #B148.
Change of MOA: intrisicresistance No data, butchange of MOA in intrinisicresistanttumorsseems plausible Motzer JCO 2009 vol. 27 (22) pp. 3584-90; EscudierLancet 2007; 370: 2103–11; Sternberg JCO 2010 vol. 28 (6) pp. 1061-8; Escudier NEJM 2007 vol. 356 (2) pp. 125-34; RixeLancetOncol 2007 vol. 8 (11) pp. 975-84
How different are VEGFR TKI really, and what is its clinical relevance? (IC50; nM) x50 x1.5 *includespretreatedpatients. **ccRCC, nephrectomy and firstlineonly 1Kumar Mol Cancer Ther2007;6(7):2012-21. 2Mendel DBClin Can Res. 2003;9:327-337. 3Wilhelm SM,Cancer Res. 2004; 64: 7099-7109. 4Wickmann et al. Proc. AACR Clin Cancer Res 2003: 44: A3780. 5J ClinOncol2007;25:884-896. 5Nosov ESMO 2010
TKI may aggregate tumor-invasiveness ...angiogenesis inhibitors targeting the VEGF pathway demonstrate antitumor effects... [in pancreatic NEC & GBM] ... concomitantly elicit tumor adaptation and progression to stages of greater malignancy, with heightened invasiveness and in some cases increased lymphatic and distant metastasis.
VEGF – a dynamic Marker of targetinhibition Murukesh British Journal of Cancer (2010) 102, 8 – 18
VEGFR-TKI treatment is associated with upregulation of PlGF Stage I-II NSCLC patients, 2-6 weekspazopanibprior to tumorresection Nikolinakos et al. Cancer Research 70(6) 2010
Angiogenic switch – a mechanism of resistence during VEGF-depletion Jubb et al.Nature Reviews Cancer 13 July 2006
VEGF-inhibitionisassociatedwithvesselmaturation • red: pericytes (SMA). green: CD31 Verheul Clin Cancer Res 2007
Everolimus inhibitsvesselmaturation in mice pericytes vessels Lane Clin Cancer Res 2009
Follow-upafter Everolimus therapy Everolimus continued (n = 3) Everolimus (N = 39) Re-exposure (40%) BSC (n = 21) Sorafenib (53%) Sunitinib (33%) Bevacizumab (7%) Subsequent therapy (n = 15) Other (7%)
OSpatientswithsubsequenttherapy (at start of everolimus) P<0.0001 OS 23.3 mo 10.9 mo P 0.0128
Is there another set of data supporting this observation?(french patients from RECORD-1) • TKI after everolimus: sunitinib 15 pts, sorafenib 11 pts, TKI258 3 pts N=36 (29evaluable) * At start of everolimus Blesius et al ESMO 2010 .
TKI-resistanceis transient in TKI-responsivepatients Patientsreceived sunitinib up-front, subsequently an mTORi and immediate re-exposure to sunitinib aftermTORi-failure Unpublisheddata
Conclusion • Sequential treatment has been adopted in the clinic • Everolimus is a valid option in TKI-refractory RCC • Resistance to TKI remains transient in responding patients and re-exposure seems suitable • Incorporation of the prevailing mechanisms of resistance into the process of treatment-decision may really advance the field • Selection of patients susceptible for either TKI or mTORi are urgently needed