Thyroid Disorders
480 likes | 654 Vues
Thyroid Disorders. G. A. (Jahan) Mozaffarian, M.D., F.A.C.P. Clinical Professor of Medicine University of Washington Jan. 25-2011 Jan. 11, 2010 5-12-2006. Thyroid Case Histories, J. S. In 1980, this 38 y/o woman was referred to our office.

Thyroid Disorders
E N D
Presentation Transcript
Thyroid Disorders G. A. (Jahan) Mozaffarian, M.D., F.A.C.P. Clinical Professor of Medicine University of Washington Jan. 25-2011 Jan. 11, 2010 5-12-2006
Thyroid Case Histories, J. S. • In 1980, this 38 y/o woman was referred to our office. • Symptoms: Heart palpitation, heat intolerance, decreased menstrual flow, insomnia & nervousness. • PMH. Rheumatic heart disease as a child and aortic stenosis. Meds: Pen-V-K, 1/day. • Exam. Pulse 110 & regular. She had tremor in hands & fingers, restlessness & heart murmur of A. S. Her thyroid was enlarged, estimated 45 gm (Nl 12 gm, non-palpable).
Dignosis • She has hyperthyroidism, probably Graves disease (as named after the Irish physician who first described this illness in modern times).
Treatment options include: Radioactive Iodine, orally. Propylthiouracil (PTU), or methimazole, orally. Surgery Symptomatic Treatment: Beta Blockers, Diazepam Hospitalization & IV fluids in significantly ill patients, …
Thyroid Case Histories, J. S. • Treatment options are discussed are discussed & she is placed on: • Propylthiouracil, 400 mg/day • Propranolol, 10 mg TID • Diazepam (at bedtime for insomnia). • She asks how long does she • need to take these medications.
J. S., Treatment • She was told that duration of treatment with PTU, or methimazole (Tapazole) is usually 2 years. • Her free thyroxine index normalizes and her symptoms subside in about 3 to 4 months. • Propranolol & diazepam were stopped after about 3 to 4 months. • TSH rose to the upper margin of normal. • PTU was gradually tapered and finally stopped after 2 years of treatment.
Thyroid Case Histories, J.S. • Since 1982, (through 2010), she has remained in excellent remission, without any evidence of relapse or recurrence. • Her thyroid has become non-palpable. • Her serum TSH has remained normal, as measured annually. • In July 2004, at age 62, she had open heart surgery in Swedish Med. Ctr., & received a porcine aortic valve prosthesis, uneventfully. • Preoperatively, her TSH was normal, & has remained normal till the present time, 2010.
Thyroid Case Histories, J.S. • In conclusion, this patient was treated with PTU for 2 years. • Treatment with PTU induced a remission which has lasted 28 years. • Duration of treatment with PTU, or methimazole is often about 2 years. This is usually adequate to produce long term remission or cure.
Hyperthyroidism Case of S. S.
Thyroid Case Histories, S. S. • This 39 year old woman was referred to our office in 1990. • She had signs & symptoms of hyperthyroidism. • Serum TSH was suppressed. • Free thyroxine (FT4) was elevated. • Treatment with oral medications, radioactive iodine or surgery is discussed. • She prefers to be treated with radioactive iodine.
SS • A radioiodine uptake test is ordered • This test would differentiate between hyperthyroidism (high values) and thyroiditis (low values). • It also helps to determine the dose. • Her thyroid uptakeis: @ 6 hr, 32% ( Nl 6%-26%) @ 24 hr, Pt 62% (Nl 8%-35%) • These high results are consistent with hyperthyroidism.
Thyroid Case Histories, S. S. • In 1990, she receives 12 mCi of I-131 po. • Treatment with I-131 could takes an average of 3 to 4 months to work. • Is any other treatment needed in the time interval?
Thyroid Case Histories, S. S. • She was placed on propylthiouracil (PTU) 400mg/day, and propranolol 10 mg TID. • Her signs and symptoms improved over the next 3 to 4 months. • Laboratory tests normalized in 6 months. • Medications were tapered & stopped • But we continued to monitor her serum TSH.
S. S. • In 1991, one year after treatment with I-131 and PTU, her symptoms have all resolved. • But, she complains of cold intolerance, constipation, facial puffiness, and fatigue. • What is the diagnosis? • What should we do?
S. S. 1990-2010 • Her serum TSH is now 20 uu/ml (Nl, 3.5-5.5). • She is placed on levothyroxine 100 mcg/day, po. • On levothyroxine treatment, she has remained clinically euthyroid. • Her serum TSH levels have remained normal in the past 20 years (1990-2010).
Thyroid Case Histories, S. S. • In conclusion, this patient was treated with radioactive iodine & PTU. • One year later, she became hypothyroid. • On levothyroxine replacement therapy, she has remained euthyroid, clinically & by laboratory testing, since 20 years ago.
Risks & Benefits of These Treatment Options • Pills • I-131 • Surgery
Adverse Reactions to Antithyroid Medications Allergic reactions to methimazole or PTU occur in 4 of 1000 cases. It is generally accepted that if a patient is allergic to one drug, the other drug could be prescribed. Both of these medications are derivatives of thiourea, initially extracted from cabbage. These two medications are chemically distinct. Cross allergy between PTU & methimazole occurs at about 15%.
Adverse Reactions of Antithyroid Medications Skin reactions are benign, per se. But, they are important signals that more serious allergic reactions may ensue. Agranulocytosis can occur, leading to infection and serious sepsis. Irreversible or fatal liver failure can occur, also. A “stat” CBC will show if agranulocytosis is present. If one quickly stopped the medication, the adverse reactions are almost always reversible.
Dr. ………………..Patient’s: Mr. H. H. Hyperthyroid 2004 Neck Street, 98004.Date: 1- 1-2004 _________________________________________________________________ Propylthiouracil (PTU), 50 mg tab Take 8 tab. PO, daily #300 tablets. If you have any fever or sore throat, stop this pill & call us. ================================================= Refills: ……….times DEA No……………
Failure of PTU or Methimazole Treatment • Treatment failures, (lack of response, or evidence of relapse or recurrence) are often due to: • Inadequate dosing, • Early tapering of medications, • Or, early withdrawal.
Possible Risks of Treatment with I-131 I-131 is administered orally & is tasteless & odorless. Often one time treatment is adequate. Absolutely contraindicated in pregnancy. Be sure patient is not pregnant (treatment or test), Hypothyroidism is the only known side effect. It occurs: 50% in 10 years, 75% in 20 years and probably 100% in longer follow-ups.
Safety Of Treatment With I-131 • There are anecdotal reports of cancer (but not well documented). • Safety record has been excellent over the past 50 years. • Use is most probably safe in children who have thyrotoxicosis.
Radioactive Iodine I131 Treatment of Hyperthyroidism • Rate & rapidity by which the patient achieves remission or cure • And the rate & rapidity of developing hypothyroidism, • Will depend on the dose.
Hyperthyroidism, Symptoms • In 82%-98%: Nervousness and Anxiety, Excessive Sweating, Heat Intolerance, Heart Palpitation, Arrhythmia, Fatigue, Weakness, Weight Loss & Hair Loss. • In 32%-65%: Insomnia, Malaise, Muscle Weakness, Eye Symptoms, Increased Number of Bowel Movements, Pretibial Edema, or Periorbital Edema • In 1%-3%: Skin Itching, Psychiatric Manifestations
Hyperthyroidism, Signs • In~90%-100%: Tachycardia. Goiter. Warm or hot skin. Moist palms. Weight loss. Tremor in outstretched hands & fingers. • In~70%: Muscle wasting (temples). Eye changes. • In ~40%: Wide pulse pressure. • In~10%: Atrial fibrillation>other arrhythmias, & cardiomegaly. • Rarely: Lymphadenopathy. Splenomegaly. Gynecomastia. Itching.
Eye Changes of Graves’ Disease Exophthalmus: unilateral, bilateral, symmetrical, or asymmetrical.Watery Eyes, ConjunctivitisStare, Ptosis, Lid Lag or Lid RetractionParesis of Extraocular Muscles, DiplopiaInability to Close Eyes
Hyperthyroidism, CCx • Cardiomegaly • Cardiac arrhythmia • & atrial fibrillation • Congestive heart failure • Muscle atrophy / weakness • Hyperkalemia or hypokalemia • Hyper- or hypokalemic periodic paralysis
In Conclusion: • Hyperthyroidism is potentially a fatal disease. • Serum TSH is the best screening test. • Serum T4, serum T3 & radioactive iodine tests will be elevated. • Treatment options include: propylthiouracil (PTU), methimazole, radioactive iodine & surgery. • Radioactive iodine treatment will nearly always lead to hypothyroidism • With proper treatment patients will do well and live a normal life.
Function Tests Serum TSH is probably the most sensitive and the best function test in the diagnosis of any thyroid disorder. Serum TSH is probably the best test to evaluate the result of any treatment in any thyroid disorder.
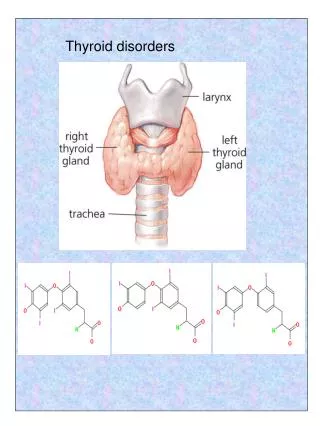
Thyroid Tests Significance • T3 uptake test, or T3 resin uptake test, or T3 % binding • Total thyroxine (T4) • Free thyroxineindex (FT4I), or Free T4 (T4) • Anti-TPO (thyroid peroxidase) antibody Or anti-TG (thyroglobulin) antibody • It measures number of unoccupied serum protein-binding sites1 • Measures free & bound T4 • It is a calculated number that estimates concentration of free T4 • Useful in diagnosis of thyroiditis. • These antibodies can give “false-positive” ANA 1. Stockigt JR. In: Werner and Ingbar’s The Thyroid, 7th ed. 1996:377. 2. NACB. Standards of Laboratory Practice. 1996.
Hypothyroidism, Hypercholesterolemia • This 13 y/o girl was referred from Olympia, WA, because of short stature. Her height was below the 3d percentile. • PMH: Hypercholesterolemia since 3 years ago & had been treated with a cholesterol lowering agent since 2 years ago. • She had no goiter, eye signs, dry skin or other signs to suggest thyroid dysfunction. • In school, she was doing really well, mostly a “A” student.
Hypothyroidism, Hypercholesterolemia • 13 y/o girl • Her TSH was > 100 uu/ml. Serum T3 & T4 were low. • She was treated with levothyroxine. • Hypercholesterolemia resolved. • Cholesterol lowering medications were stopped. • In the next 2 years, she grew 2 inches taller.
Conclusion • Initial evaluation of hyperlipidemia or hypercholesterolemia should always include a serum TSH testing.
Myxedematous Coma This elderly patient, came to the ER, Cherry Hill Campus,, in coma and was admitted to the ICU.
Myxedematous Coma • Coma • Dry skin • Hypothermia • Bradycardia • Cardiomegaly & Bradycardia • High morbidity, 50% mortality • Use triiodothyronine (T3) via NG tube if possible • Treat with IV thyroxine 0.1 mg q 4 hr. to 12 hr. in the first 24-48 hr.
Myxedematous Coma This elderly patient, came to the ER, Cherry Hill Campus,, in coma and was admitted to the ICU.
Treated With IV levothyroxine (T4) and NG tube liothyronine (T3)
It took approximately 6 weeks before she regained her level of conciousness to any meaningful degree
Treatment of Hypothyroidism, Choices: • T4, levothyroxine (Synthroid) • T3 liothyronine (Cytomel) • Or a combination.
Pregnancy, Hypo or Hyperthyroidism • See the patient monthly. • Measure TSH monthly. • Keep the TSH in the normal range. This is of utmost importance. • Serum TSH is a much more reliable test than T4, T3, & free T3 or freeT4.
Thyroid Gland Examination • Inspect the neck form the front, resting and upon swallowing. • Stand behind the patient and palpate the thyroid resting and upon swallowing. • Listen with the bell of the stethoscope for a bruit which if present is almost pathognomonic of hyperthyroidism.