IODINE
IODINE . Goiter has been known since the days of Lord Buddha and before. Earliest evidence of goiter: 3000 BC. Framework . History Sources of iodine Mechanism Daily requirements Spectrum of IDD Assessment of iodine National Iodine deficiency disorders control program. HISTORY.

IODINE
E N D
Presentation Transcript
Goiter has been known since the days of Lord Buddha and before Earliest evidence of goiter: 3000 BC
Framework • History • Sources of iodine • Mechanism • Daily requirements • Spectrum of IDD • Assessment of iodine • National Iodine deficiency disorders control program
HISTORY • In 1811 Bernard Curtois discovered iodine. • During that time Napoleon’s army needed larger quantity of the gunpowder. • The basic component of the gunpowder was niter, which production requires bigger amount of wooden ashes. • Since the war lasted for a long time, and woods eligible for logging, burning and making gunpowder were disappearing fast, so seaweeds were burned. • Making niter, Curtois accidentally added too much of sulfuric acid, and purple cloud of condensated gas has shown on the radiator, forming glistening crystals. BERNARD CURTOIS
Curtoisrealized that he has created something new and started to examine that. • Governmental resources were overloaded by Napoleon’s wars, so there was no money for further experiments. • Finally Humphry Davy on December 10th in 1813 named this element IODINE after Greek word “purple color ”. HUMPHRY DAVY
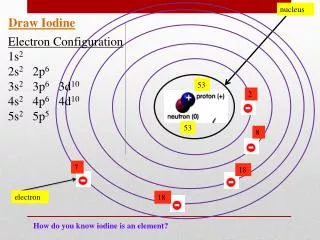
What is iodine? • Iodine is an essential micronutrient supporting some of the most vital functions of the human body. • Iodine is a nutrient needed in a minute quantity daily.Recommended daily intake: 150 μg • Total quantity present in body is (15-20 mg)mostly in thyroid gland
Iodine : Daily requirements [WHO, UNICEF, ICCIDD: Recommended iodine levels in salt and guidelines for monitoring their adequacy and effectiveness. WHO/NUT/96.13. Geneva. 1996 ]
Sources of iodine • Vegetables grown on iodine-rich soils. • Seafood • Dairy products • Eggs • Cereal grains • Legumes • Green leaves(spinach) • Water
Loss of iodine Iodine deficiency is endemic in the mountainous areas with poor soil content such as the sub-Himalayan regions. This is due to iodine being washed from the soil.
Assessment of iodine nutrition • Thyroid size by palpation and/or by ultrasonography, • Urinary Iodine (UI) excretion • Neonatal serum TSH screening for hypothyroidism • Serum thyroglobulinconcentation.
National iodine deficiency disorders control program • Following the successful trial of iodised salt in Kangra valley, Himachal Pradesh in 1962, India has launched 100% centrally sponsored the National Goitre Control Programme. • In 1992, the National Goitre Control Programme (NGCP) was renamed as National Iodine Deficiency Disorder Control Programme(NIDDCP).
Objectives 1.Surveys to assess the magnitude of the Iodine Deficiency Disorders. 2.Supply of Iodated salt in place of common salt. 3.Resurvey after every 5 Years to assess the extent of Iodine Deficiency Disorders and the impact of iodated salt. 4.Laboratory monitoring of iodated salt in urinary iodine excretion. 5.Health education. Strategies: The recommended strategy for IDD control is based on correcting the deficiency by increasing iodine intake through supplementation or food fortification.
Iodine supplementation The first iodine supplements were in the form of an oral solution of iodine such as Lugol, which was given daily. After the Second World War, considerable progress was made in reducing IDD with iodized oil – initially using the intramuscular form and in the 1990s, using the oral form
The oral form of iodized oil has several advantages over the intramuscular form: • it does not require special storage conditions or trained health personnel for the injection • it can be given once a year. • Compared to iodized salt, however, it is more expensive and coverage can be limited since it requires direct contact with each person. • With the introduction of iodized salt on a large scale, iodized oil is now only recommended for populations living in severely endemic areas with no access to iodized salt.
Food fortification with iodine • The World Health Assembly adopted universal salt iodization (USI) as the method of choice to eliminate IDD. • In 2002, at the Special Session on Children of the United Nations (UN) General Assembly, the goal to eliminate IDD by the year 2005 was set. • USI was chosen as the best strategy based on the following facts: • Salt is one of the few commodities consumed by everyone • Salt consumption is fairly stable throughout the year • Salt production is usually in the hands of few producers • USI is easy to implement & available at a reasonable cost • The addition of iodine to salt does not affect its colour, taste or odour • The quality of iodized salt can be monitored at the production, retail and household levels • Salt iodization programmes are easy to implement.
In order to meet the iodine requirements of a population it is recommended to add 20 to 40 parts per million (ppm) of iodine to salt (assuming an average salt intake of 10 g per capita/day) . • There are two forms of iodine fortificants, Potassium iodate Potassium iodide. • Pottasiumiodate is more stable under extreme climatic conditions it is preferred to iodide, especially in hot and humid climates . • North America and some European countries use potassium iodide while most tropical countries use potassium iodate.
Criteria for monitoring process towards sustainable IDD elimination
References • WHO, UNICEF, ICCIDD. Assessment of iodine deficiency disorders and monitoring their elimination. Geneva, World Health Organization, 2001 (WHO/NHD/01.1). • Walter F, Boron . "SYNTHESIS OF THYROID HORMONES" in: Medical Physiology: A Cellular And Molecular Approach. Elsevier/Saunders.2003.48 :1300. Available fromISBN1-4160-2328-3 • http://www.nihfw.org/NDC/DocumentationServices/NationalHealthProgramme/NATIONALIODINEDEFICIENCYDISORDERS.html • Government of Maharashtra, public health department. Directorate of health services http://www.mahaarogya.gov.in/projectandschemes/default.htm • Iodine status worldwide .WHO Global Databaseon Iodine Deficiency.2004 • Andersson M et al .Global Iodine Status and Trends over the Past Decade .2011.