Pediatric lymphoblastic lymphomas
370 likes | 580 Vues
Pediatric lymphoblastic lymphomas. Beirut 14/10/ 2011. NHL in Children. NHL : 10% of Pediatric Cancers Lymphoblastic Lymphomas : 30%-35% Immunophenotype T(80%), Very rare diseases : INTERNATIONAL COLLABORATION. Lymphoblastic Lymphomas. Clinical characterisitics Diagnosis Prognosis

Pediatric lymphoblastic lymphomas
E N D
Presentation Transcript
Pediatric lymphoblastic lymphomas Beirut 14/10/ 2011
NHL in Children • NHL : 10% of Pediatric Cancers • Lymphoblastic Lymphomas : 30%-35% • Immunophenotype T(80%), • Very rare diseases : INTERNATIONAL COLLABORATION
Lymphoblastic Lymphomas • Clinical characterisitics • Diagnosis • Prognosis • Treatment • Perspectives
I CLINICAL MANIFESTATIONS 1. T-cell LL • Mediastinal involvement +++, : dyspnea, cough, vascular compression, edema • Pleural effusion, • Cervical, axillary adenopathies,
II CLINICAL MANIFESTATIONS 2. preB-LL: • Bone lesions • Skin, subcutaneous tissue • Lymph nodes • testis • other
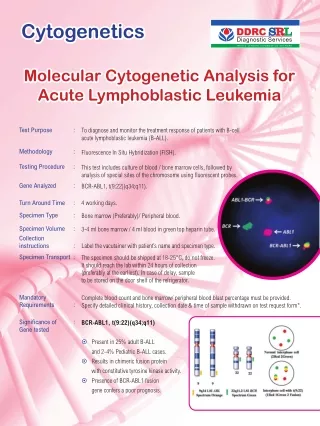
II Diagnosis and staging • Diagnosis: Cyto puncture, biopsy • Cytologic exam, immunophenotyping, cytogenetics and molecular analysis • CT scan • Bone marrow analysis ( 2 sites) and CSF examination • Other exams according to the site of the disease • Staging : St Jude’s classification
Lymphoblastic lymphomas . Immunophenotype • CD34, TdT, HLA-DR • B LL : CD79a, (c/s)CD22,CD19, CD10, cIgm, sIg • T LL : (c/s)CD3, CD7, • CD2, CD5, CD1a, • CD10, CD4, CD8, TCR
EGIL classification of lymphoblastic lymphomas T LL T1 (proT) = Tdt, CD3 cyt , CD7 T2 (preT) = Tdt, CD3 cyt, CD7, CD2 , CD5 T3 (cortical) = Tdt, CD3 cyt, CD7, CD2, CD5, CD1a+,CD4±, CD8± → better steroid response and better prognosis T4 (mature) = Tdt, CD1a-, CD4± or CD8±, CD3 TCRαβ+ TCRγδ+ Pre B LL B1 (proB) = Tdt, HLADR, CD19, CD22 et CD79a B2 (common) = Tdt, HLADR, CD19, CD22, CD79a et CD10 B3 (preB) = + µ cytoplasm B4 (mature) = Tdt ±, + Ig membran or kappa/lambda cyt
Molecular analysis T LL • TCR gene rearrangement • Classification : • Immature, more frequent in adults (LYL1 and LMO2 expression) • Intermediate , with expression of HOXA9, and CALM-AF10 or NUP214-ABL rearrangement • Mature
Immature, sCD3-, bF1- Pre-ab, sCD3-, bF1+ TCR+, sCD3+ T-LL classification • TCR based classification « ab-LBL » TCRddelg+b+ « IM0/d LBL » TCRdDJ/-g-b- « Int. LBL » TCRd+g+b+ TCR+ Pre- (cTCRb +) IM(cTCRb -) selection ? IMg IMb IM0 IMd TCR+ pT/ cTCRb + ? TCR+ pT - Good prognosis Poor prognosis Poor prognosis Retrospective study : 32 adults, 9 children Baleydier et al., Clin. Cancer Research 2008
Immature, sCD3-, bF1- Pre-ab, sCD3-, bF1+ TCR+, sCD3+ Oncogenetic abnormalities in T-LL • Small series in T-LL as compared to T cell ALL « ab-LBL » TCRddelg+b+ « IM0/d LBL » TCRdDJ/-g-b- « Int. LBL » TCRd+g+b+ TCR+ Pre- (cTCRb +) IM(cTCRb -) selection ? IMg IMb IM0 IMd TCR+ pT/ cTCRb + ? TCR+ pT - LYL1, LMO2 TLX1 (8%), HOXA9 (32%) CALM-AF10, NUP-ABL ? Other events ? Baleydier et al., Clin. Cancer Research 2008
Sex Age >10 years Stage LDH> 2N Immunophénotype D33 response Induction/consolidation response ns ns ns ns ns ns ns III Pediatric T-LLPrognostic factors
More recent prognostic factors • Poorer prognosis for girls >9 ans ( Burkhardt et al BJH 2005) • Poor prognosis cytogenetics : del 6q14-24 (Burkhardt et al Leukemia 2006) • Molecular datas ?
Chromosome 6q alterations • Loss of heterozygoty at 6q14-24 : poor prognosis (Burkhardt et al Leukemia 2006,20,1422-29): 61/18 - LOH 6q : 13/18 relapses and 5/41 patients in CR1 Recently, it was confirmed on a new series of patients (B Burkhardt : oral communication)
Notch1 and FBXW7 mutations in T-LL • 54 pts treated according to EURO LB 02 • 55% Notch1 and or FBXW7 mutations : better EFS and survival • 7% absence of biallellic TCRγ deletion : very poor prognosis C. Callens et al submitted
T ALL/ T LL • BM > or<25% • WHO classification : T lymphoblastic leukaemia/lymphoma • Treatment : ALL strategy
T ALL and T-LL • T-ALL, prognosis depends on : • Prephase response : corticoïsteroids and 1 IT MTX • Minimal residual disease after induction/consolidation • Which is the better way to define such criteria for T-LL ?
MDD/MRD • Flow cytometry and RQ-PCR : MDD and MRD (blood and BM) • Prognostic value of MDD(Coustan-Smith JCO 2009): EFS < with BM involvement (1 à 5%) : 68% vs 90% at 2 years. • But …… • Prospective studies mandatory . European protocols : same EFS for patients with stage III and IV
MDD/MRD • Value of blood samples for the follow-up (flow cytometry): • Coustan-Smith JCO 2009 : 30 pts : - 19 pts negative at D7 - 11 pts positive (2 pts relapsed in the BM) - Stark Ped Blood Cancer 2009 : 17 pts - MDD at diagnosis > 80% - MRD at J33 (10 pts) : 1 pt > 10-2 : relapse
IV Treatment • CHEMOTHERAPY ONLY, derived from T-ALL protocols with cure >80% • No surgery • No radiotherapy
European protocol EURO LB02 • Why ? • > 80% patients cured from a rare disease • Better characterization of prognosis factors, with stratification of patients on risk factors Consensus for BFM 90 without radiotherapy as reference arm
EURO-LB 02 NHL-BFM 90 Stage I+II Induction Protocole M P Maintenance 6-MP/MTX Cranial RT Induction Protocole M III+IV P ReInduction Maintenance 104 Semaine 1 9 11 19 21 28 30
EURO-LB-02 Re-Induction except stades I+II Induction Maintenance Consoli- dation 24 months 6-MP/MTX I/1-PRED P Random 1 I/2 M Prot. II Random 2 I/1-DEXA 6-MP/MTX 18 months Precursor-T-cell-LBL: Randomisation 1+2
Randomisations(1) • Dexamethasone/predniso(lo)ne • Better efficacy in vitro (Kaspers MPO 1996) • Better CSF concentration for DEXA • Better efficacy in some trials, but … • Toxicity : infectious ? Osteonecrosis ? • Optimal Dose of dexa ?
Randomisation (2) 2. Lenght of the treatment : 24 months vs 18 months Local and early relapses
Conclusions • Better prognosis with polychemotherapy • Relapses : early and localized • Cranial radiotherapy should be avoided • Prognosis factors to be determined for better stratification of the patients • Prospective evaluation of TEPscan • International collaboration mandatory (protocols and biological evaluation) • New therapeutic modalities (Notch inhibitors, nelarabine, monoclonal antibodies…)