Chronic HIV Infection
430 likes | 553 Vues
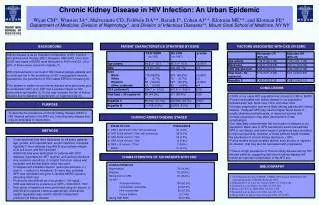
This overview discusses chronic HIV infection, its clinical manifestations, and the importance of monitoring CD4 count and viral load throughout different stages of the disease. It highlights common symptoms, such as fever and weight loss, and outlines the recommended prophylactic treatments against prevalent opportunistic infections like Pneumocystis carinii pneumonia (PCP), Toxoplasmosis, and Tuberculosis. The article emphasizes the need for careful management and early intervention based on individual patient CD4 levels and the identification of unexplained syndromes.

Chronic HIV Infection
E N D
Presentation Transcript
Chronic HIV Infection Clinical Manifestations Opportunistic Infections O.I. Prophylaxis
CD4 Count, Viral Load and Clinical Course Primary Infection Sero-conversion Intermediate Stage AIDS CD4 Cell Count Plasma RNA Copies 1,000 CD4 Cells 500 4-8 Weeks Up to 12 Years 2-3 Years
Common Clinical Manifestations of Chronic HIV Infection • Constitutional Symptoms • fever • weight loss/wasting • fatigue • Organ/System Specific • virtually all organ systems can be affected • Consider HIV testing for unexplained syndromes
Wasting By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
Prophylaxis against Opportunistic Infections • Pneumocystis carinii pneumonia (PCP) • Toxoplasmosis gondii • Mycobacterium Avium Complex (MAC) • Cryptococcal Meningitis • CMV retinitis • Mycobacterium tuberculosis (TB)
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
PCP - Primary Prophylaxis • Initiate at CD4<200 or prior AIDS-defining illness • Best: TMP-SMX • 1 DS qd, 1 SS qd, 1 DS qod or tiw • 1 DS qd also confers protection vs T. gondii and common bacterial infections • consider desensitization if allergic reaction • up to 70% of patients can tolerate reinstitution of therapy
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
Toxoplasmic Encephalitis Primary Prophylaxis • Avoid contact with cat feces, raw or undercooked meat, esp. if IgG (-) • Initiate primary prophylaxis at CD4<100 • Options include: • TMP-SMX • dapsone plus pyrimethamine/leucovorin • atovaquone plus pyrimethamine/leucovorin • pyrimethamine-sulfadiazine/leucovorin
MAC Primary Prophylaxis • initiate at CD4<50; R/O dMAC first if symptomatic • options: • clarithromycin 500mg po bid • azithromycin 500mg po qd or 1200mg po qwk • rifabutin 300mg po qd • survival benefit shown for clarithromycin • multiple interactions between rifabutin and antiretrovirals
Cytomegalovirus Primary Prophylaxis • Counseling and regular ophthalmological exams for patients with CD4<50 • CMV(-) blood for patients who are CMV(-) at baseline
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
Candidal Infections • fluconazole can reduce risk of vaginal, oropharyngeal and esophageal infection • however, generally not recommended: • potential for resistance, cost, possibility of drug interactions • low mortality associated with these infections • acute treatment generally effective
Candidal Infections for which prophylaxis may be warranted: • recurrent esophageal candidiasis: fluconazole 100-200mg qd • recurrent Candida vaginitis: weekly intravaginal clotrimazole tablets or lactobacillus gel capsules reduces frequency by approximately 50%1 1. Abstract 677, 7th Conference on Retroviruses and Opportunistic Infections, 2000.
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
Tuberculosis Prophylaxis: Treatment of Latent TB Infection PPD > 5 mm IndurationorRecent Contact with Infectious TB Patient *Rifampin600 mg qd x 2 monthsplusPyrazinamide20 mg/kg/d x 2 months Isoniazid300 mg qd x 9 months or 900 mg 2x/week x 9 months *Use Rifabutin 300 mg qd if patient on PI From: CDC. MMWR 1999;48:No. RR-10. DHS/OI/PP
Consultation Services for Clinicians Caring for Patients with HIV/AIDS • Northwest AETC • (206) 994-8773 pager, (206) 731-1058 VM • University of Washington MEDCON • (800) 326-5300 • National HIV Telephone Consultation Service (Warmline) • (800) 933-3413 • National Clinicians’ Post-Exposure Prophylaxis Hotline (PEPline) • (888) HIV-4911
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
Primary Prophylaxis vs Cryptococcal Meningitis? • Fluconazole provides limited protection • resistance can develop • Not routinely recommended