Procedural and Diagnosis Coding Based on Documentation
Procedural and Diagnosis Coding Based on Documentation. How much to document?. Presenter Disclosures. Jean Troop. “No relationships to disclose”. The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months:.

Procedural and Diagnosis Coding Based on Documentation
E N D
Presentation Transcript
Procedural and Diagnosis Coding Based on Documentation How much to document? SCHA-MI Annual Meeting 2014
Presenter Disclosures Jean Troop “No relationships to disclose” The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months: SCHA-MI Annual Meeting 2014
Session Objectives: CPT • E&M Code Requirements ICD 10 • Code Assignment • Documentation Requirements Putting it Together SCHA-MI Annual Meeting 2014
Revenue Maximization Strategies • Identify the services you provide and pair those with appropriate procedure code • Encounter form/Super-bill/Route slip • Provide education on how to choose appropriate services SCHA-MI Annual Meeting 2014
CPT Levels of Service • Review the components that make up an E&M Level • Key components • History • Exam • Medical Decision Making • Contributing Factors • Presenting problem • Counseling • Coordination of care • Face to face time SCHA-MI Annual Meeting 2014
History Levels • Problem Focused • Expanded problem focused • Detailed • Comprehensive SCHA-MI Annual Meeting 2014
Examination Types • Problem focused • Expanded problem focused • Detailed • Comprehensive SCHA-MI Annual Meeting 2014
Medical Decision Making • Type of Medical decision making • Number of diagnoses or management options • Amount and/or complexity of data to be reviewed • Risk of complications and/or morbidity or mortality SCHA-MI Annual Meeting 2014
ICD 10 CM • How many of you have had some training in ICD 10 CM? • How many are a part of your fiduciary or health systems ICD 10 CM committee/project team/plan? • What level of understanding or comfort level are you currently at with ICD 10 CM? • Beginner • Intermediate • Advanced • Expert SCHA-MI Annual Meeting 2014
Why Change? • ICD 9 needed revisions • Improved ability to identify risk and severity • Better reflects current medical practices • Ability to capture specific data from clinical documentation • Facilitate patient care coordination across settings • Allows for improved public health reporting and tracking • Allows for better quality outcome reporting SCHA-MI Annual Meeting 2014
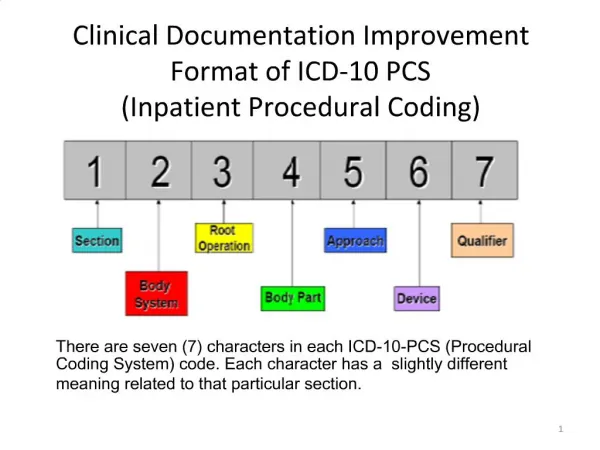
ICD 10 CM-Structure • 3 – 7 Characters in length • Characters can be alpha or numeric • All codes begin with an alpha-character • 2nd character is numeric • 3rd thru 7th characters can be alpha or numeric • Placeholders are used if 7th character is required and code is less than 6 characters (x = placeholder) SCHA-MI Annual Meeting 2014
ICD 10 CM Code Structure continued… • First 3 characters form the category code • Category codes are main entry within the tabular list • Category code may be further expanded by etiology, severity, site, manifestations or intent all within the 4th thru 6th characters • 7th character is an extension required in some categories to further defines the episode of care, status of fracture healing, the number of fetus in obstetrical conditions or the site of recording of the Glasgow coma scale SCHA-MI Annual Meeting 2014
ICD 10 CM Book Format • Alpha index • Alphabetical listing of terms • Neoplasm Table • Table of Drugs and Chemicals • External Causes Index • Tabular List • 21 Chapters • Sequential alpha-numeric list of codes • includes indented listing of categories, subcategories and codes • Contains instructional notes and conventions SCHA-MI Annual Meeting 2014
Accurate Code Selection 3 steps to accurate code selection: • Look up diagnosis or condition in alpha index • Read all instructional notes and look at the conventions • In tabular list, check for instructions at the 3-digit category level , subcategory level and code level • Why is this important? SCHA-MI Annual Meeting 2014
Documentation & Coding go hand-in-hand • Documentation supports: • Patient care/Care coordination • Medical necessity • Coding and reimbursement • Compliance • Increased specificity in ICD-10 may require documentation changes SCHA-MI Annual Meeting 2014
Increased Granularity How do the changes affect documentation? • Increased site specificity • Laterality (right, left or bilateral) • Episode of care (initial, subsequent, sequela) • Increased specificity related to type of injury • Lifestyle habits (alcohol, tobacco or drug abuse or dependence) SCHA-MI Annual Meeting 2014
Examples for Documentation Changes SCHA-MI Annual Meeting 2014
Factors influencing health status and contact for health services…Chapter 21 • AMA/CPT Defines: Z codes represent reasons for encounters. A corresponding procedure code must accompany a Z code if a procedure is performed. Categories Z00-Z99 are provided for occasions when circumstances other than a disease, injury or external cause classifiable to categories A00-Y89 are recorded as 'diagnoses' or 'problems'. This can arise in two main ways: • (a) When a person who may or may not be sick encounters the health services for some specific purpose, such as to receive limited care or service for a current condition, to donate an organ or tissue, to receive prophylactic vaccination (immunization), or to discuss a problem which is in itself not a disease or injury. • (b) When some circumstance or problem is present which influences the person's health status but is not in itself a current illness or injury. SCHA-MI Annual Meeting 2014
Immunizations and other health conditions • Immunizations require just one diagnosis code: • Z23 –Encounter for immunization • In addition there is now a code to report under-immunization status • X28.3—Under-immunization status • Category Z77 indicates contact with or suspected exposure to substance that are known to be hazardous to health. • Z77.22—Exposure to tobacco smoke (second hand smoke) SCHA-MI Annual Meeting 2014
Screening • Use of screening versus signs and symptoms • Testing to rule out a suspected diagnosis is not screening—use signs and symptoms to explain • Screening is testing for disease or disease precursors in seemingly well individuals for early detection • First listed diagnosis versus additional code • Screening code may be first-listed if the reason for the visit is specifically screening exam • Screening can be secondary if the screening is done during a visit for other health problem • Should a condition be discovered during the screening then the code for that condition may be assigned as an additional (secondary) diagnosis SCHA-MI Annual Meeting 2014
Let’s code it! • Provider documented that the patient is being seen for preventative exam. On this visit, the provider notes that the patient has an elevated blood pressure of 150/96 which has not been present on previous visits. He/she wants to determine if this is an isolated finding or if the patient has hypertension and requests that the patient return for blood pressure checks. Identify the correct assignment and sequencing of the ICD-10-CM diagnosis codes: Hypertension: I10 Elevated Blood Pressure: R03.0 Routine exam: Z00.121 (w/abnormal finding) or Z00.129 (w/o abnormal finding) a. Z00.129, I10 b. R03.0 , Z00.121 c. Z00.121, R03.0 d. I10, Z00.121 SCHA-MI Annual Meeting 2014
Code This: • Established patient comes in with a chief complaint of headaches. States symptoms have been present for a few days and Advil is not helping. ROS is limited to affected area. Provider performs an limited exam of head and listens to the lungs. • What is our level of service? • What is our Diagnosis code? • Could/Should we have documented anything differently? SCHA-MI Annual Meeting 2014
Coding for Annual PE • 12 year old established patient comes in for routine PE. No abnormal findings. HPV and Flu vaccines were given. Procedure Code: Diagnoses: SCHA-MI Annual Meeting 2014
Otitis Media • Documentation Requirement.pdf • Laterality • Status (acute versus chronic) • Specify type • Exposure to our use of tobacco SCHA-MI Annual Meeting 2014
ICD-10 Resources • http://www.cms.gov/Medicare/Coding/ICD10/ProviderResources.html • http://www.cms.gov/Medicare/Coding/ICD10/ICD-10ImplementationTimelines.html • http://www.cms.gov/Medicare/Coding/ICD10/MedicaidResources.html SCHA-MI Annual Meeting 2014
Thank you for your time today • If you would like additional information please feel free to contact us we are here to help. • Jean Troop, MBA, RHIT jtroop@scha-mi.org or • Susette Bader-Sherwood ssherwood@scha-mi.org SCHA-MI Annual Meeting 2014